Karas Patrick J, Giridharan Nisha, Treiber Jeffrey M, Prablek Marc A, Khan A Basit, Shofty Ben, Krishnan Vaishnav, Chu Jennifer, Van Ness Paul C, Maheshwari Atul, Haneef Zulfi, Gavvala Jay R, Sheth Sameer A
Department of Neurosurgery, Baylor College of Medicine, Houston, TX, United States.
Department of Neurology, Comprehensive Epilepsy Center, Baylor College of Medicine, Houston, TX, United States.
Front Neurol. 2020 Dec 10;11:590825. doi: 10.3389/fneur.2020.590825. eCollection 2020.
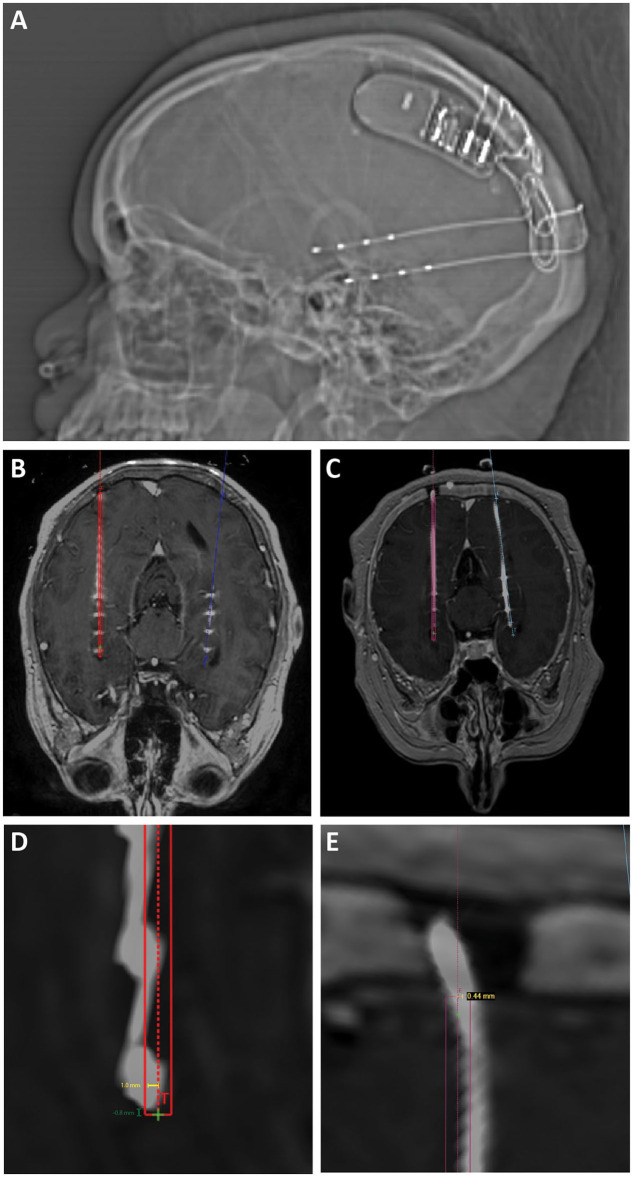
Robotic stereotaxy is increasingly common in epilepsy surgery for the implantation of stereo-electroencephalography (sEEG) electrodes for intracranial seizure monitoring. The use of robots is also gaining popularity for permanent stereotactic lead implantation applications such as in deep brain stimulation and responsive neurostimulation (RNS) procedures. We describe the evolution of our robotic stereotactic implantation technique for placement of occipital-approach hippocampal RNS depth leads. We performed a retrospective review of 10 consecutive patients who underwent robotic RNS hippocampal depth electrode implantation. Accuracy of depth lead implantation was measured by registering intraoperative post-implantation fluoroscopic CT images and post-operative CT scans with the stereotactic plan to measure implantation accuracy. Seizure data were also collected from the RNS devices and analyzed to obtain initial seizure control outcome estimates. Ten patients underwent occipital-approach hippocampal RNS depth electrode placement for medically refractory epilepsy. A total of 18 depth electrodes were included in the analysis. Six patients (10 electrodes) were implanted in the supine position, with mean target radial error of 1.9 ± 0.9 mm (mean ± SD). Four patients (8 electrodes) were implanted in the prone position, with mean radial error of 0.8 ± 0.3 mm. The radial error was significantly smaller when electrodes were implanted in the prone position compared to the supine position ( = 0.002). Early results (median follow-up time 7.4 months) demonstrate mean seizure frequency reduction of 26% ( = 8), with 37.5% achieving ≥50% reduction in seizure frequency as measured by RNS long episode counts. Prone positioning for robotic implantation of occipital-approach hippocampal RNS depth electrodes led to lower radial target error compared to supine positioning. The robotic platform offers a number of workflow advantages over traditional frame-based approaches, including parallel rather than serial operation in a bilateral case, decreased concern regarding human error in setting frame coordinates, and surgeon comfort.
在癫痫手术中,机器人立体定向技术越来越普遍地用于植入立体脑电图(sEEG)电极以进行颅内癫痫监测。机器人在永久性立体定向导联植入应用中也越来越受欢迎,例如在深部脑刺激和反应性神经刺激(RNS)手术中。我们描述了用于枕下入路海马RNS深度导联放置的机器人立体定向植入技术的演变。我们对10例连续接受机器人RNS海马深度电极植入的患者进行了回顾性研究。通过将术中植入后透视CT图像和术后CT扫描与立体定向计划进行配准来测量深度导联植入的准确性,以测量植入准确性。还从RNS设备收集癫痫发作数据并进行分析,以获得初始癫痫发作控制结果估计。10例患者因药物难治性癫痫接受了枕下入路海马RNS深度电极放置。分析共纳入18个深度电极。6例患者(10个电极)仰卧位植入,平均目标径向误差为1.9±0.9mm(平均值±标准差)。4例患者(8个电极)俯卧位植入,平均径向误差为0.8±0.3mm。与仰卧位相比,俯卧位植入电极时径向误差明显更小(P = 0.002)。早期结果(中位随访时间7.4个月)显示癫痫发作频率平均降低26%(P = 0.08),通过RNS长时间发作计数测量,37.5%的患者癫痫发作频率降低≥50%。与仰卧位相比,机器人植入枕下入路海马RNS深度电极的俯卧位导致更低的径向目标误差。与传统的基于框架的方法相比,机器人平台具有许多工作流程优势,包括双侧病例中的并行而非串行操作、减少设置框架坐标时人为误差的担忧以及外科医生的舒适度。