Univ. Lille, U1286-INFINITE-Institute for Translational Research in Inflammation, Lille, France.
Inserm, Lille, France.
Front Immunol. 2020 Dec 18;11:558811. doi: 10.3389/fimmu.2020.558811. eCollection 2020.
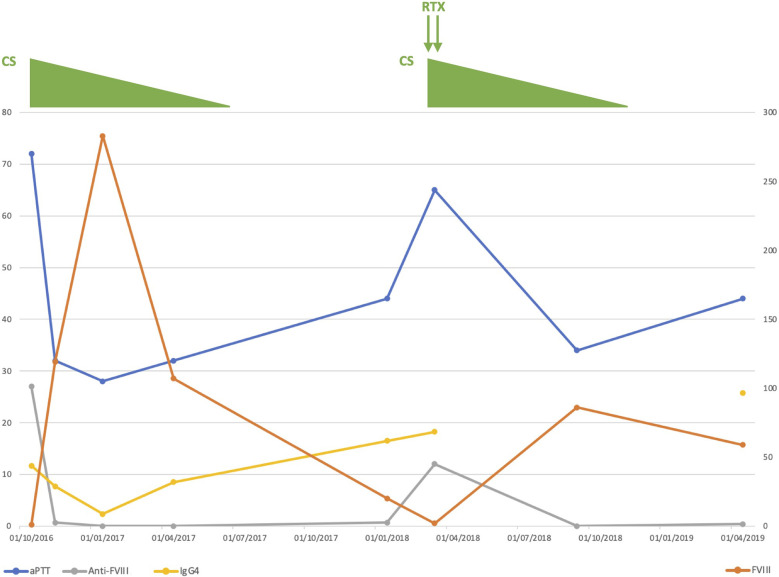
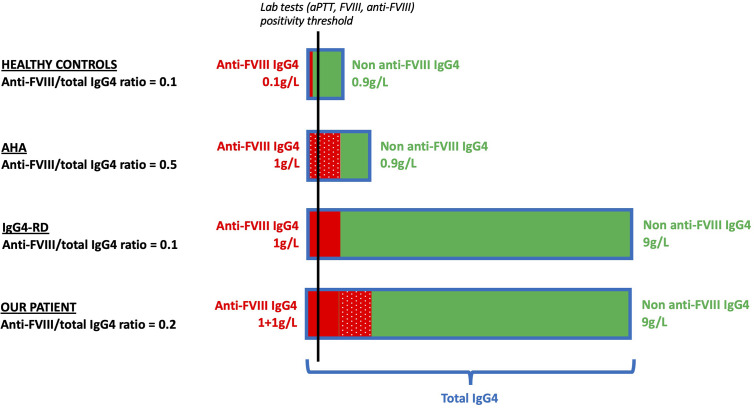
We report the observation of a 75-year-old patient referred for cervical lymphadenopathies. A pre-lymphadenectomy blood work revealed an asymptomatic elevation of aPTT with low factor VIII (FVIII) levels and high anti-FVIII antibodies titers, consistent with acquired hemophilia A (AHA). Histological work-up of a cervical lymphadenopathy revealed benign follicular hyperplasia with IgG4 lymphoplasmacytic infiltration; and serum IgG4 levels were markedly elevated, compatible with IgG4-related disease (IgG4-RD). He was successfully treated with a 9-month course of prednisone, secondarily associated with rituximab when an AHA relapse occurred. As this patient presented with an unusual association of rare diseases, we wondered whether there was a link between the two conditions. Our first hypothesis was that the anti-FVIII autoantibodies could be directly produced by the proliferating IgG4 plasma cells as a result of broken tolerance to autologous FVIII. To test this assumption, we determined the anti-FVIII IgG subclasses in our patient and in a control group of 11 AHA patients without IgG4-RD. The FVIII inhibitor was mostly IgG4, with an anti-FVIII IgG4/IgG1 ratio of 42 at diagnosis and 268 at relapse in our patient; similar values were observed in non-IgG4-RD AHA patients. As a second hypothesis, we considered whether the anti-FVIII activity could be the result of a non-specific autoantibody production due to polyclonal IgG4 plasma cell proliferation. To test this hypothesis, we measured the anti-FVIII IgG4/total IgG4 ratio in our patient, as well as in several control groups: 11 AHA patients without IgG4-RD, 8 IgG4-RD patients without AHA, and 11 healthy controls. We found that the median [min-max] ratio was higher in AHA-only controls (2.4 10 [5.7 10-1.79 10]), an oligoclonal setting in which only anti-FVIII plasma cells proliferate, than in IgG4-RD-only controls (3.0 10 [2.0 10-6.0 10]), a polyclonal setting in which all IgG4 plasma cells proliferate equally. Our patient had intermediate ratio values (2.7 10 at diagnosis and 1.0 10 at relapse), which could plead for a combination of both mechanisms. Although no definitive conclusion can be drawn, we hypothesized that the anti-FVIII autoantibody production in our IgG4-RD AHA patient could be the result of both broken tolerance to FVIII and bystander polyclonal IgG4 plasma cell proliferation.
我们报告了一例 75 岁患者因颈部淋巴结病就诊的情况。淋巴结切除术前的血液检查显示,活化部分凝血活酶时间(aPTT)升高,因子 VIII(FVIII)水平降低,抗 FVIII 抗体滴度升高,符合获得性血友病 A(AHA)。颈部淋巴结病的组织学检查显示良性滤泡性增生伴 IgG4 淋巴浆细胞浸润;血清 IgG4 水平显著升高,符合 IgG4 相关疾病(IgG4-RD)。患者接受了 9 个月的泼尼松治疗,当出现 AHA 复发时,联合使用利妥昔单抗。由于该患者表现出罕见疾病的不常见关联,我们想知道这两种情况之间是否存在联系。我们的第一个假设是,抗 FVIII 自身抗体可能是由于对自身 FVIII 的耐受性丧失而由增殖的 IgG4 浆细胞直接产生的。为了验证这一假设,我们测定了我们患者和 11 名无 IgG4-RD 的 AHA 患者对照组的抗 FVIII IgG 亚类。FVIII 抑制剂主要是 IgG4,在患者诊断时为 42,复发时为 268;非 IgG4-RD AHA 患者也观察到类似的数值。作为第二个假设,我们考虑抗 FVIII 活性是否是由于多克隆 IgG4 浆细胞增殖导致的非特异性自身抗体产生的结果。为了验证这一假设,我们测量了患者以及以下对照组的抗 FVIII IgG4/总 IgG4 比值:11 名无 IgG4-RD 的 AHA 患者、8 名无 AHA 的 IgG4-RD 患者和 11 名健康对照者。我们发现,仅 AHA 对照组(中位数 [最小-最大]:2.4 10 [5.7 10-1.79 10])的比值较高,这是一个仅增殖抗 FVIII 浆细胞的寡克隆状态,而 IgG4-RD 对照组(中位数 [最小-最大]:3.0 10 [2.0 10-6.0 10])的比值较低,这是一个所有 IgG4 浆细胞均增殖的多克隆状态。我们的患者具有中间比值(诊断时为 2.7 10,复发时为 1.0 10),这可能支持两种机制的结合。尽管不能得出明确的结论,但我们假设 IgG4-RD AHA 患者的抗 FVIII 自身抗体产生可能是由于对 FVIII 的耐受性丧失和旁观者多克隆 IgG4 浆细胞增殖所致。