Xiao Ming-Hu, Wu Yong-Jian, Wang Jing-Jin, Song Guang-Yuan, Wang Jian-De, Zhu Zhen-Hui, Wang Xu, Zhao Zhen-Yan, Wang Hao
Department of Echocardiography, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
J Geriatr Cardiol. 2020 Dec 28;17(12):766-774. doi: 10.11909/j.issn.1671-5411.2020.12.006.
The effective orifice area (EOA) is utilized to characterize the hemodynamic performance of the transcatheter heart valve (THV). However, there is no consensus on EOA measurement of self-expanding THV. We aimed to compare two echocardiographic methods for EOA measurement following transcatheter self-expanding aortic valve implantation.
EOA was calculated according to the continuity equation. Two methods were constructed. In Method 1 and Method 2, the left ventricular outflow tract diameter (LVOTd) was measured at the entry of the prosthesis (from trailing-to-leading edge) and proximal to the prosthetic valve leaflets (from trailing-to- leading edge), respectively. The velocity-time integral (VTI) of the LVOT (VTI) was recorded by pulsed-wave Doppler (PW) from apical windows. The region of the PW sampling should match that of the LVOTd measurement with precise localization. The mean transvalvular pressure gradient (MG) and VTI of THV was measured by Continuous wave Doppler.
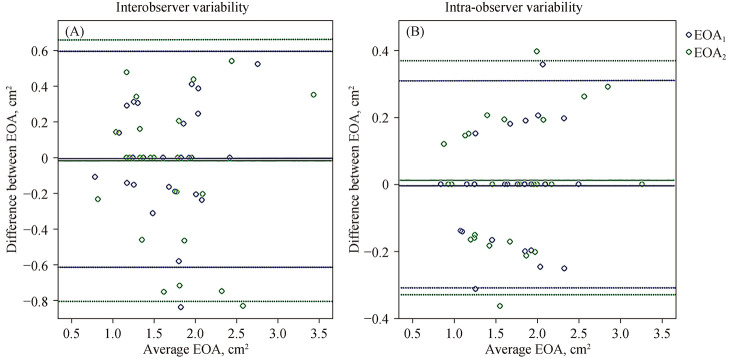
A total of 113 consecutive patients were recruited. The mean age was 77.2 ± 5.5 years, and 72 patients (63.7%) were male. EOA with the use of Method 1 was larger than EOA (1.56 ± 0.39 cm 1.48 ± 0.41 cm, = 0.001). MG correlated better with the indexed EOA (EOAI) ( = -0.701, < 0.001) than EOAI ( = -0.645, < 0.001). According to EOAI (EOAI ≤ 0.65 cm/m, respectively), the proportion of sever prosthesis-patient mismatch with the use of EOA was lower than EOA (12.4% 21.2%, < 0.05). Compared with EOA, EOA had lower interobserver and intra-observer variability (intra: 0.5% ± 17% 3.8% ± 22%, < 0.001; inter: 1.0% ± 9% 3.5% ± 11%, < 0.001).
For transcatheter self-expanding valve EOA measurement, LVOTd should be measured in the entry of the prosthesis stent (from trailing-to-leading edge), and VTI should match that of the LVOTd measurement with precise localization.
有效瓣口面积(EOA)用于表征经导管心脏瓣膜(THV)的血流动力学性能。然而,对于自膨胀式THV的EOA测量尚无共识。我们旨在比较经导管自膨胀主动脉瓣植入术后两种超声心动图测量EOA的方法。
根据连续性方程计算EOA。构建了两种方法。在方法1和方法2中,左心室流出道直径(LVOTd)分别在假体入口处(从后缘到前缘)和人工瓣膜小叶近端(从后缘到前缘)测量。通过心尖窗的脉冲波多普勒(PW)记录LVOT的速度时间积分(VTI)。PW采样区域应与LVOTd测量区域精确匹配。通过连续波多普勒测量THV的平均跨瓣压差(MG)和VTI。
共纳入113例连续患者。平均年龄为77.2±5.5岁,72例患者(63.7%)为男性。使用方法1测得的EOA大于EOA(1.56±0.39 cm对1.48±0.41 cm,P = 0.001)。MG与指数化EOA(EOAI)的相关性更好(r = -0.701,P < 0.001),而不是EOAI(r = -0.645,P < 0.001)。根据EOAI(EOAI≤0.65 cm/m²),使用EOA时严重人工瓣膜-患者不匹配的比例低于EOA(12.4%对21.2%,P < 0.05)。与EOA相比,EOA的观察者间和观察者内变异性更低(观察者内:0.5%±17%对3.8%±22%,P < 0.001;观察者间:1.0%±9%对3.5%±11%,P < 0.001)。
对于经导管自膨胀瓣膜的EOA测量,LVOTd应在假体支架入口处(从后缘到前缘)测量,VTI应与LVOTd测量精确匹配。