Cupisti Adamasco, Giannese Domenico, Moriconi Diego, D'Alessandro Claudia, Torreggiani Massimo, Piccoli Giorgina B
Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Néphrologie, Centre Hospitalier Le Mans, Le Mans, France.
Front Med (Lausanne). 2020 Dec 3;7:622593. doi: 10.3389/fmed.2020.622593. eCollection 2020.
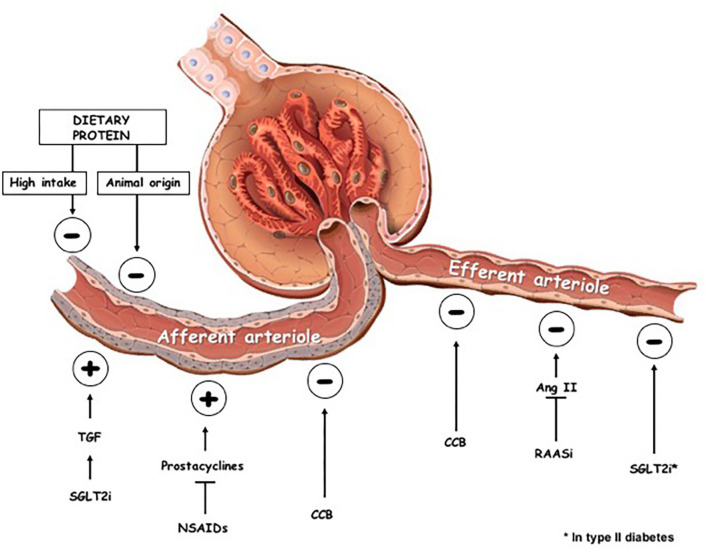
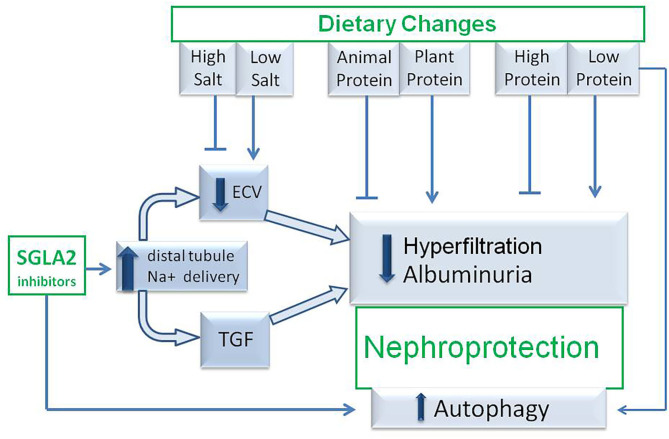
Sodium-glucose-transporter 2 inhibitors (SGLT2i) are a new class of anti-diabetic drugs that in large trials such as CREDENCE have shown also a reduction of glomerular hyperfiltration and albuminuria in type 2 diabetic patients. Hence, the interest toward SGLT2i is focused toward this potential nephroprotective effect, in order to reduce the progression to overt nephropathy, and it seems to be confirmed in the most recent DAPA-CKD trial. This is the reason why the indication for SGLT2i treatment has been extended to chronic kidney disease (CKD) patients with eGFR up to 30 ml/min, namely with CKD stage 1-3. In patients with CKD stage 3 to 5, the most recent KDIGO guidelines recommend low-protein diet and plant-based regimens to delay end-stage kidney disease (ESKD) and improve quality of life. Similarly to SGLT2i, low-protein diets exert renal-protective effects by reducing single nephron hyperfiltration and urinary protein excretion. Beyond the glomerular hemodynamic effects, both protein restriction and SGLT2i are able to restore autophagy and, through these mechanisms, they may exert protective effects on diabetic kidney disease. In this perspective, it is likely that diet may modulate the effect of SGLT2i in CKD patients. Unfortunately, no data are available on the outcomes of the association of SGLT2i and low-protein and/or vegan diets. It is therefore reasonable to investigate whether CKD patients receiving SGLT2i may have further advantages in terms of nephroprotection from the implementation of a low-protein and/or plant-based diet or whether this association does not result in an additive effect, especially in vascular nephropathies.
钠-葡萄糖协同转运蛋白2抑制剂(SGLT2i)是一类新型抗糖尿病药物,在诸如CREDENCE等大型试验中已表明,其还可降低2型糖尿病患者的肾小球高滤过和蛋白尿。因此,对SGLT2i的关注集中在这种潜在的肾脏保护作用上,以减少向显性肾病的进展,并且这似乎在最近的DAPA-CKD试验中得到了证实。这就是SGLT2i治疗适应证已扩展至估算肾小球滤过率(eGFR)高达30 ml/min的慢性肾脏病(CKD)患者(即CKD 1-3期患者)的原因。对于CKD 3至5期患者,最新的KDIGO指南推荐低蛋白饮食和植物性饮食方案,以延缓终末期肾病(ESKD)并改善生活质量。与SGLT2i类似,低蛋白饮食通过减少单个肾单位的高滤过和尿蛋白排泄发挥肾脏保护作用。除了肾小球血流动力学效应外,蛋白质限制和SGLT2i都能够恢复自噬,并且通过这些机制,它们可能对糖尿病肾病发挥保护作用。从这个角度来看,饮食可能会调节SGLT2i在CKD患者中的作用。不幸的是,目前尚无关于SGLT2i与低蛋白和/或纯素饮食联合应用效果的数据。因此,研究接受SGLT2i治疗的CKD患者在实施低蛋白和/或植物性饮食后是否在肾脏保护方面有进一步的优势,或者这种联合应用是否不会产生叠加效应,尤其是在血管性肾病中,是合理的。