Petrella Francesco, Radice Davide, Guarize Juliana, Piperno Gaia, Rampinelli Cristiano, de Marinis Filippo, Spaggiari Lorenzo
Department of Thoracic Surgery, IRCCS European Institute of Oncology, 20141 Milan, Italy.
Department of Oncology and Hemato-Oncology, Università degli Studi di Milano, 20141 Milan, Italy.
Cancers (Basel). 2021 Jan 10;13(2):228. doi: 10.3390/cancers13020228.
the aim of this paper is to quantify multidisciplinary team meeting (MDT) impact on the decisional clinical pathway of thoracic cancer patients, assessing the modification rate of the initial out-patient evaluation.
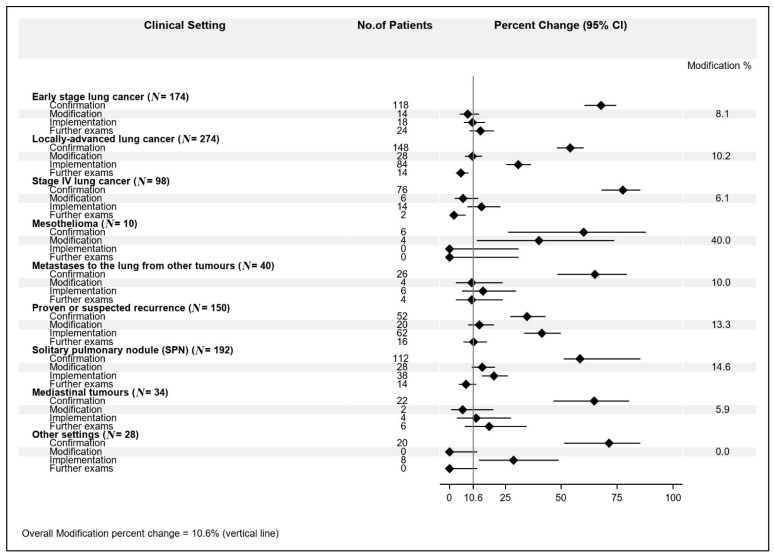
the impact of MDT was classified as follows: confirmation: same conclusions as out-patient hypothesis; modification: change of out-patient hypothesis; implementation: definition of a clear clinical track/conclusion for patients that did not receive any clinical hypothesis; further exams required: the findings that emerged in the MDT meeting require further exams.
one thousand consecutive patients evaluated at MDT meetings were enrolled. Clinical settings of patients were: early stage lung cancer (17.4%); locally advanced lung cancer (27.4%); stage IV lung cancer (9.8%); mesothelioma (1%); metastases to the lung from other primary tumors (4%); histologically proven or suspected recurrence from previous lung cancer (15%); solitary pulmonary nodule (19.2%); mediastinal tumors (3.4%); other settings (2.8%).
MDT meetings impact patient management in oncologic thoracic surgery by modifying the out-patient clinical hypothesis in 10.6% of cases; the clinical settings with the highest decisional modification rates are "solitary pulmonary nodule" and "proven or suspected recurrence" with modification rates of 14.6% and 13.3%, respectively.
本文旨在量化多学科团队会议(MDT)对肺癌患者决策临床路径的影响,评估初始门诊评估的修改率。
MDT的影响分类如下:确认:与门诊假设结论相同;修改:门诊假设改变;实施:为未得到任何临床假设的患者确定明确的临床路径/结论;需要进一步检查:MDT会议中出现的结果需要进一步检查。
纳入了在MDT会议上评估的1000例连续患者。患者的临床情况为:早期肺癌(17.4%);局部晚期肺癌(27.4%);IV期肺癌(9.8%);间皮瘤(1%);其他原发性肿瘤肺转移(4%);经组织学证实或怀疑为既往肺癌复发(15%);孤立性肺结节(19.2%);纵隔肿瘤(3.4%);其他情况(2.8%)。
MDT会议通过在10.6%的病例中修改门诊临床假设来影响肿瘤胸外科患者的管理;决策修改率最高的临床情况是“孤立性肺结节”和“证实或怀疑复发”,修改率分别为14.6%和13.3%。