Ursaru Andreea Maria, Haba Cristian Mihai, Popescu Ștefan Eduard, Crișu Daniela, Petriș Antoniu Octavian, Tesloianu Nicolae Dan
Department of Cardiology, Emergency Clinical Hospital "Sf. Spiridon", 700111 Iași, Romania.
Department of Cardiology, "Grigore. T. Popa" University of Medicine and Pharmacy, 700115 Iași, Romania.
Diagnostics (Basel). 2021 Jan 9;11(1):96. doi: 10.3390/diagnostics11010096.
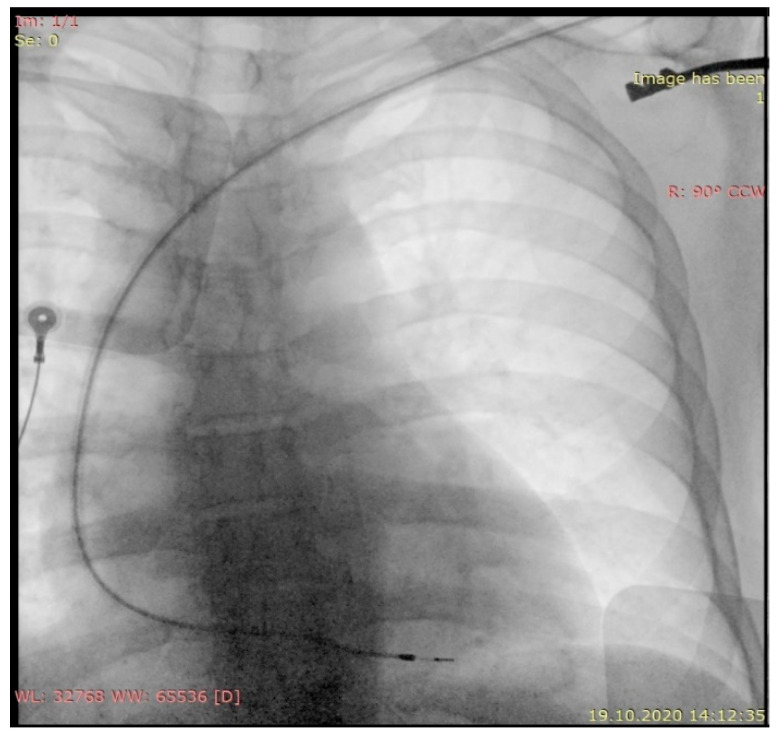
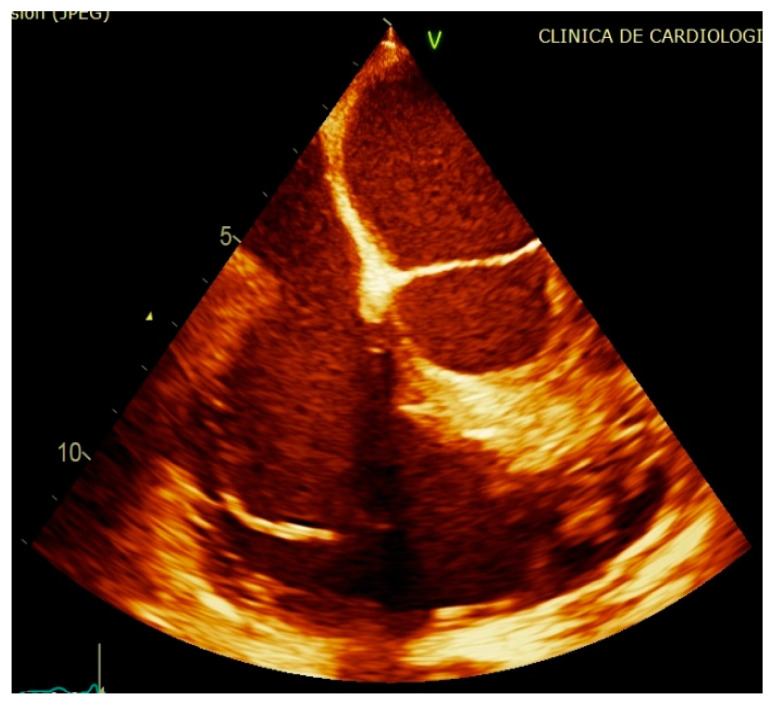
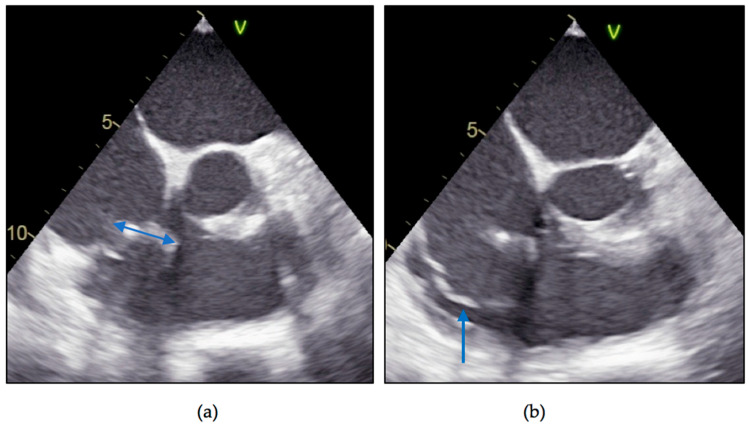
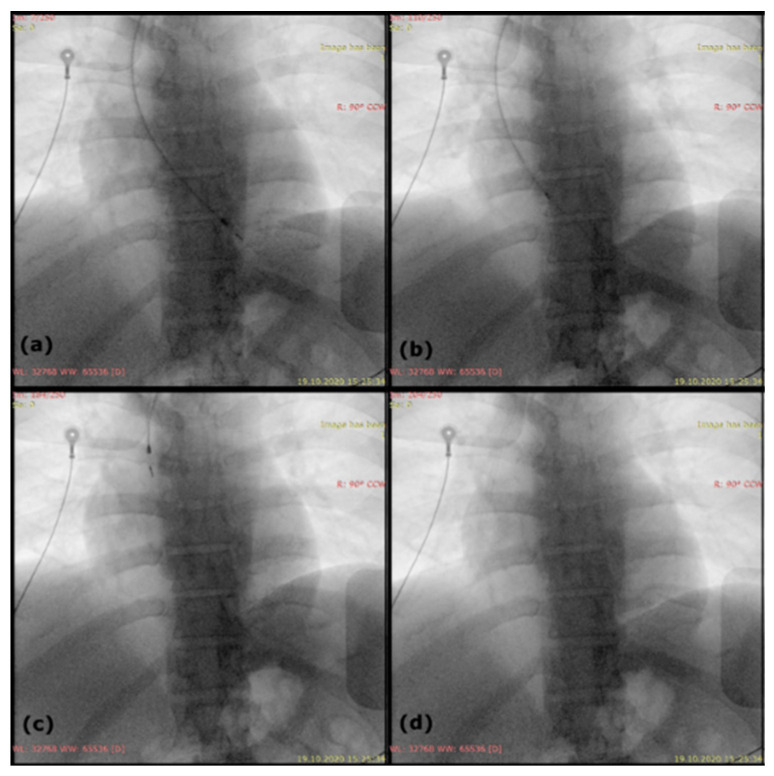
The number of infections related to cardiac implantable electronic devices (CIEDs) has increased as the number of devices implanted around the world has grown exponentially in recent years. CIED complications can sometimes be difficult to diagnose and manage, as in the case of lead-related infective endocarditis. We present the case of a 48-year-old male diagnosed with Staphylococcus aureus device-related infective endocarditis, 12 years after the implant of a single chamber pacemaker. A recent history of the patient includes two urinary catheterizations due to obstructive uropathy in the context of a prostatic adenoma, 2 months previously, both without antibiotic prophylaxis; no other possible entry sites were found and no history of other invasive procedures. After initiation of antibiotic therapy according to antibiotic susceptibility testing, we decided to remove the right ventricular passive fixation lead along with the vegetation and pacemaker generator; because of severe lead adhesions in the costoclavicular region, and especially in the right ventricle, we needed mechanical sheaths to remove the abundant fibrous tissue that encompassed the lead. After a difficult, but successful, lead extraction along with a large vegetation and 6 weeks' antibiotic therapy, the clinical and biological evolution was favorable, without reappearance of symptoms. While very late lead endocarditis is a rarity, late lead-related infective endocarditis (more than 12 months elapsed since implant) is not an exception; this is why we find that endocarditis prophylaxis should be reconsidered in certain patient categories, our patient being proof that procedures with neglectable endocarditis risk according to the guidelines can lead to bacterial endocarditis.
近年来,随着全球植入心脏植入式电子设备(CIED)的数量呈指数级增长,与CIED相关的感染数量也有所增加。CIED并发症有时难以诊断和处理,例如与导线相关的感染性心内膜炎。我们报告一例48岁男性患者,在植入单腔起搏器12年后被诊断为金黄色葡萄球菌设备相关感染性心内膜炎。患者近期病史包括2个月前因前列腺腺瘤导致梗阻性尿路病进行了两次导尿,均未进行抗生素预防;未发现其他可能的感染入口,也无其他侵入性操作史。根据抗生素敏感性试验开始抗生素治疗后,我们决定移除右心室被动固定导线、赘生物和起搏器发生器;由于锁骨下区域,尤其是右心室存在严重的导线粘连,我们需要使用机械鞘管来清除包裹导线的大量纤维组织。经过艰难但成功的导线拔除以及切除一大块赘生物,并进行了6周的抗生素治疗后,临床和生物学进展良好,症状未再出现。虽然极晚期导线心内膜炎较为罕见,但晚期导线相关感染性心内膜炎(植入后超过12个月)并不罕见;这就是为什么我们认为在某些患者类别中应重新考虑心内膜炎预防措施,我们的患者证明了根据指南心内膜炎风险可忽略不计的操作也可能导致细菌性心内膜炎。