School of Population and Public Health, University of British Columbia, 2206 E Mall, Vancouver, British Columbia, Canada.
Centre for Health Evaluation and Outcome Science, University of British Columbia, Vancouver, Canada.
BMC Med Res Methodol. 2021 Jan 13;21(1):21. doi: 10.1186/s12874-020-01198-2.
The use of individual patient data (IPD) in network meta-analyses (NMA) is rapidly growing. This study aimed to determine, through simulations, the impact of select factors on the validity and precision of NMA estimates when combining IPD and aggregate data (AgD) relative to using AgD only.
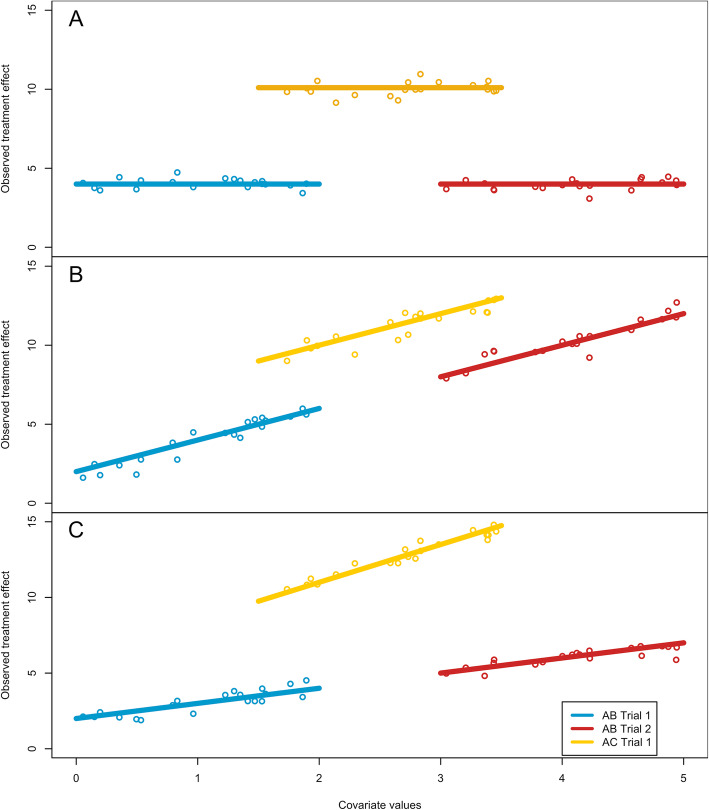
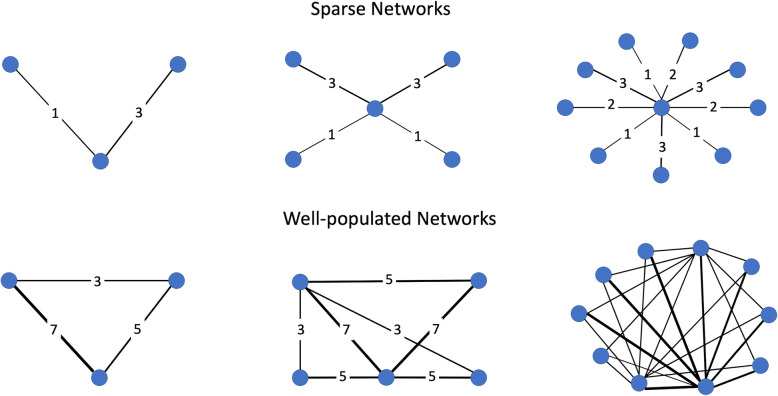
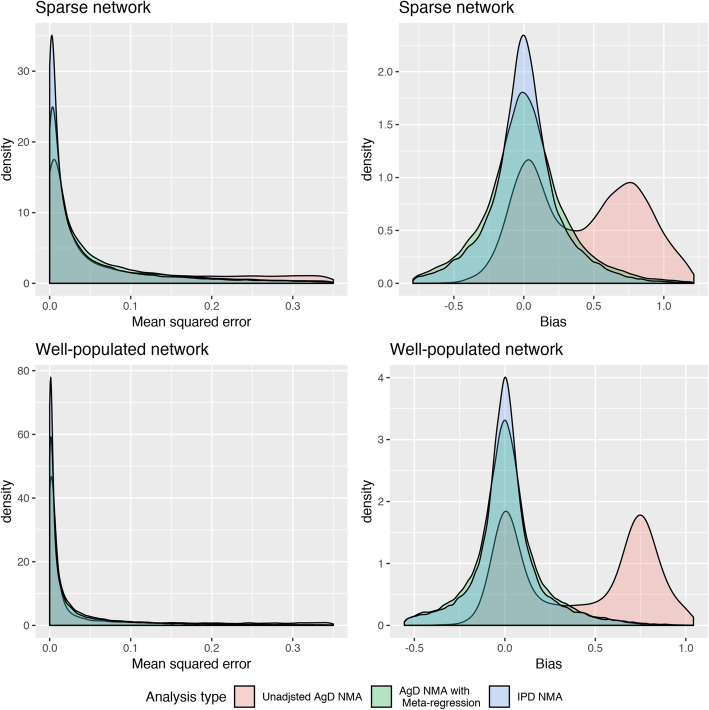
Three analysis strategies were compared via simulations: 1) AgD NMA without adjustments (AgD-NMA); 2) AgD NMA with meta-regression (AgD-NMA-MR); and 3) IPD-AgD NMA with meta-regression (IPD-NMA). We compared 108 parameter permutations: number of network nodes (3, 5 or 10); proportion of treatment comparisons informed by IPD (low, medium or high); equal size trials (2-armed with 200 patients per arm) or larger IPD trials (500 patients per arm); sparse or well-populated networks; and type of effect-modification (none, constant across treatment comparisons, or exchangeable). Data were generated over 200 simulations for each combination of parameters, each using linear regression with Normal distributions. To assess model performance and estimate validity, the mean squared error (MSE) and bias of treatment-effect and covariate estimates were collected. Standard errors (SE) and percentiles were used to compare estimate precision.
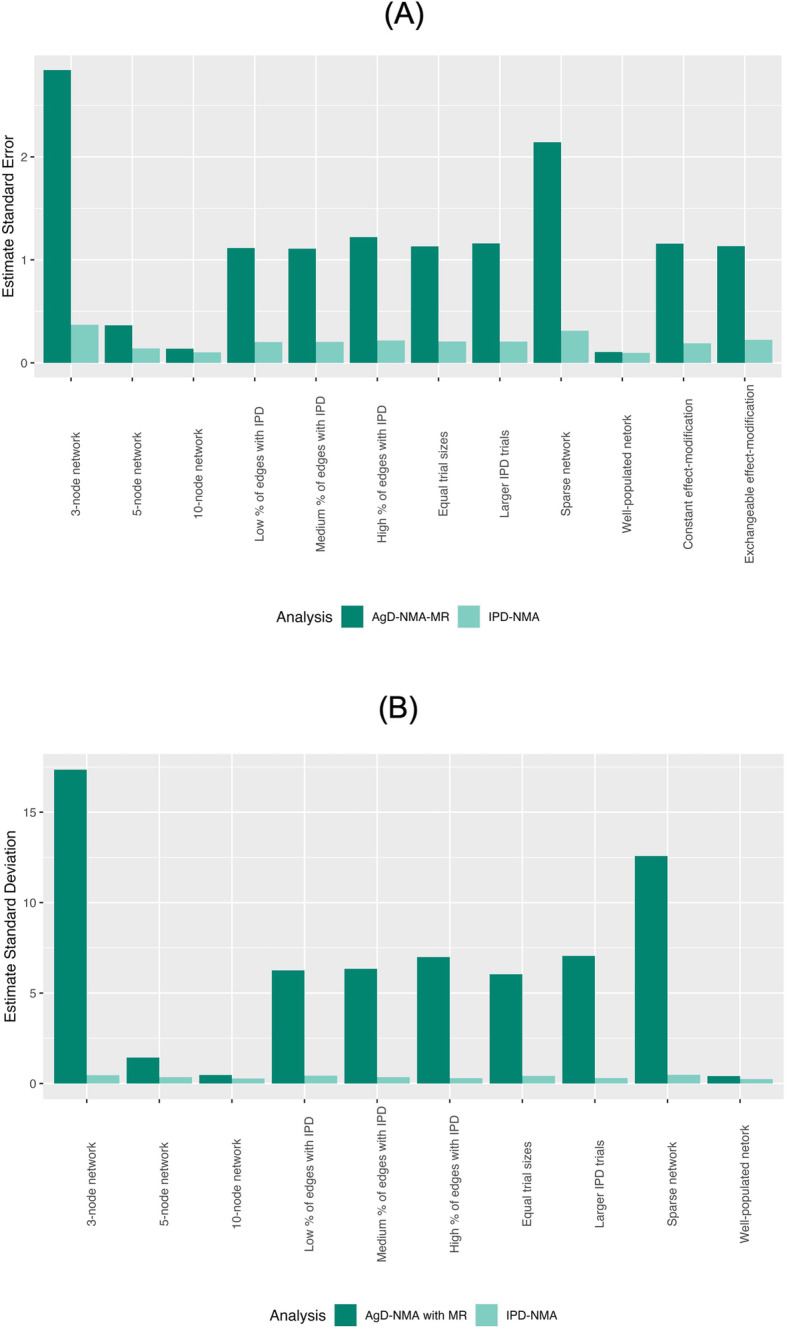
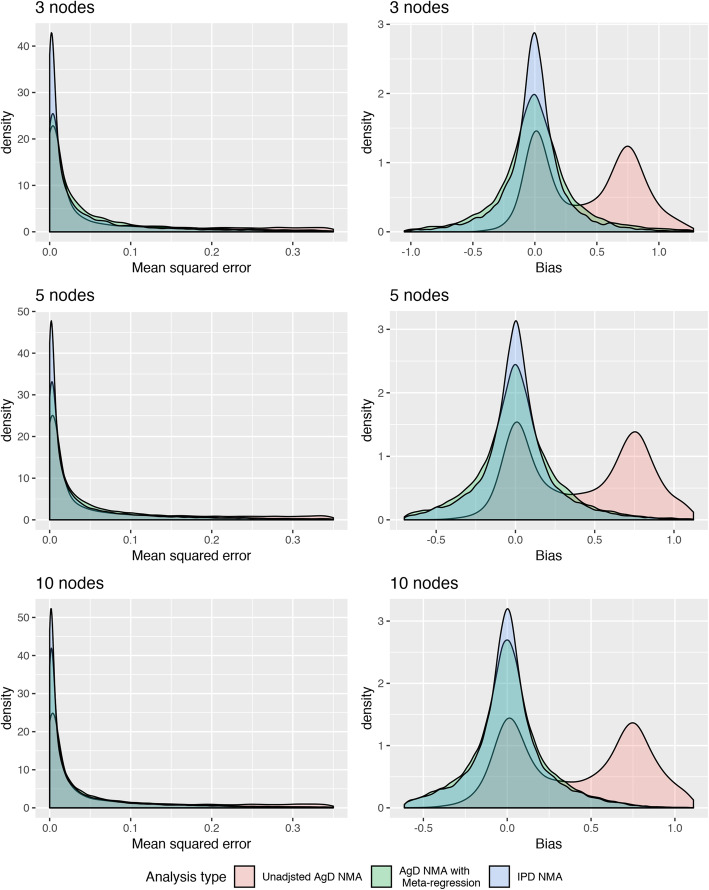
Overall, IPD-NMA performed best in terms of validity and precision. The median MSE was lower in the IPD-NMA in 88 of 108 scenarios (similar results otherwise). On average, the IPD-NMA median MSE was 0.54 times the median using AgD-NMA-MR. Similarly, the SEs of the IPD-NMA treatment-effect estimates were 1/5 the size of AgD-NMA-MR SEs. The magnitude of superior validity and precision of using IPD-NMA varied across scenarios and was associated with the amount of IPD. Using IPD in small or sparse networks consistently led to improved validity and precision; however, in large/dense networks IPD tended to have negligible impact if too few IPD were included. Similar results also apply to the meta-regression coefficient estimates.
Our simulation study suggests that the use of IPD in NMA will considerably improve the validity and precision of estimates of treatment effect and regression coefficients in the most NMA IPD data-scenarios. However, IPD may not add meaningful validity and precision to NMAs of large and dense treatment networks when negligible IPD are used.
个体患者数据(IPD)在网络荟萃分析(NMA)中的使用正在迅速增加。本研究旨在通过模拟确定,与仅使用汇总数据(AgD)相比,当组合使用 IPD 和 AgD 时,选择因素对 NMA 估计的有效性和精度有何影响。
通过模拟比较了三种分析策略:1)不进行调整的 AgD NMA(AgD-NMA);2)具有荟萃回归的 AgD NMA(AgD-NMA-MR);3)具有荟萃回归的 IPD-AgD NMA(IPD-NMA)。我们比较了 108 个参数排列:网络节点数量(3、5 或 10);由 IPD 提供信息的治疗比较比例(低、中或高);相等大小的试验(双臂,每臂 200 名患者)或更大的 IPD 试验(每臂 500 名患者);稀疏或人口密集的网络;以及效应修饰类型(无、跨治疗比较恒定或可交换)。对于每种参数组合,每种参数组合都使用正态分布的线性回归生成 200 次模拟的数据。为了评估模型性能并估计有效性,收集了治疗效果和协变量估计的均方误差(MSE)和偏差。使用标准误差(SE)和百分位数来比较估计精度。
总体而言,IPD-NMA 在有效性和精度方面表现最佳。在 108 种情况下,有 88 种情况下 IPD-NMA 的中位数 MSE 较低(否则结果相似)。平均而言,IPD-NMA 的中位数 MSE 是使用 AgD-NMA-MR 的中位数的 0.54 倍。同样,IPD-NMA 治疗效果估计的 SE 是 AgD-NMA-MR SE 的 1/5 大小。使用 IPD-NMA 的有效性和精度优势的大小因情况而异,并与 IPD 的数量有关。在小或稀疏的网络中使用 IPD 始终可以提高有效性和精度;但是,在大/密集的网络中,如果使用的 IPD 太少,则 IPD 往往不会产生太大影响。类似的结果也适用于荟萃回归系数的估计。
我们的模拟研究表明,在 NMA 中使用 IPD 将大大提高治疗效果和回归系数估计的有效性和精度,尤其是在大多数 NMA IPD 数据情况下。然而,当使用微不足道的 IPD 时,IPD 可能不会为大型和密集型治疗网络的 NMA 增加有意义的有效性和精度。