Sobrado Carlos Walter, de Almeida Obregon Carlos, Sobrado Lucas Faraco, Bassi Lucas Morales, Bacchi Hora José Américo, Silva E Sousa Júnior Afonso Henrique, Nahas Sergio Carlos, Cecconello Ivan
Colorectal Surgery Division, Department of Gastroenterology, University of São Paulo School of Medicine, São Paulo, Brazil.
Ann Med Surg (Lond). 2020 Dec 19;61:97-100. doi: 10.1016/j.amsu.2020.12.019. eCollection 2021 Jan.
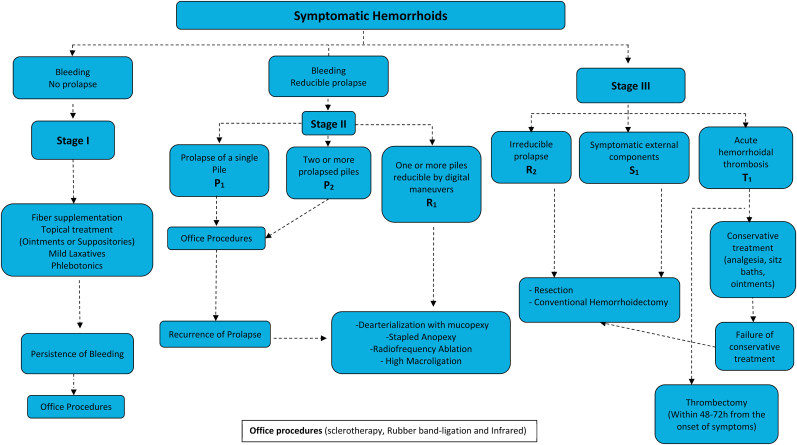
The classification for HD was developed by Goligher in 1980 and does not contemplate important aspects of this disease, which limits its use in guiding treatment. The aim of this study if to apply in clinical practice the new classification for hemorrhoids named BPRST (bleeding, prolapse, reduction, skin tags, thrombosis), to compare it with the original classification proposed by Goligher and to propose an algorithm for treatment.
This is a prospective study conducted at the University of São Paulo's teaching hospital and . Patients with HD treated from March 2011 to July 2013 were included. Patients were classified according to BPRST and Goligher classifications and treated according to personal experience and most updated guidelines. The association between both classifications and the treatment adopted was compared and an algorithm for treatment was developed.
229 patients were included in this study and 28 patients were lost due to follow-up. According to Goligher, 29, 61, 85 and 26 were classified as grades I, II, III and IV, respectively. According to the BPRST, 23 were classified as stage I, 95 as stage II and 83 as stage III. Six patients classified as Goligher I were reclassified as BPRST stage III and required conventional hemorrhoidectomy, either due to thrombosis (n = 4) or intolerable skin tags (n = 2). The BPRST classification was more closely associated with the type of treatment employed and had few outliers than Goligher (p < 0.001).
There are limitations to the use of Goligher's classification in clinical practice. The novel BPRST classification includes important aspects of HD that should be considered when deciding the best treatment option. Our algorithm for treatment contemplates the most commonly used techniques and can help to guide the treatment of this complex disease.
痔的分类由戈利格尔于1980年提出,未考虑到该疾病的重要方面,这限制了其在指导治疗中的应用。本研究的目的是将名为BPRST(出血、脱垂、回纳、皮赘、血栓形成)的痔新分类应用于临床实践,将其与戈利格尔提出的原始分类进行比较,并提出一种治疗算法。
这是一项在圣保罗大学教学医院进行的前瞻性研究。纳入2011年3月至2013年7月接受治疗的痔患者。根据BPRST和戈利格尔分类对患者进行分类,并根据个人经验和最新指南进行治疗。比较两种分类与所采用治疗之间的关联,并制定一种治疗算法。
本研究纳入229例患者,28例患者失访。根据戈利格尔分类,分别有29例、61例、85例和26例被分类为I级、II级、III级和IV级。根据BPRST分类,23例被分类为I期,95例为II期,83例为III期。6例被分类为戈利格尔I级的患者被重新分类为BPRST III期,由于血栓形成(n = 4)或难以忍受的皮赘(n = 2)而需要进行传统痔切除术。BPRST分类与所采用的治疗类型更密切相关,且异常值比戈利格尔分类少(p < 0.001)。
戈利格尔分类在临床实践中的应用存在局限性。新的BPRST分类包括了痔的重要方面,在决定最佳治疗方案时应予以考虑。我们的治疗算法考虑了最常用的技术,有助于指导这种复杂疾病的治疗。