The Sixth Department of Health Care, The Second Medical Center & National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, 100048, China.
BMC Emerg Med. 2021 Jan 14;21(1):6. doi: 10.1186/s12873-021-00402-w.
Optimization of preoxygenation procedure can help to secure the method of intubation by reducing the risks of severe hypoxemia and other problems. There is confusion for efficacy of non-invasive ventilation compared to high-flow oxygen therapy regarding occurrence of severe hypoxemia during the intubation procedure. The purpose of the study was to compare the difference between noninvasive ventilation and high flow oxygen therapy to prevent desaturation during laryngoscopy.
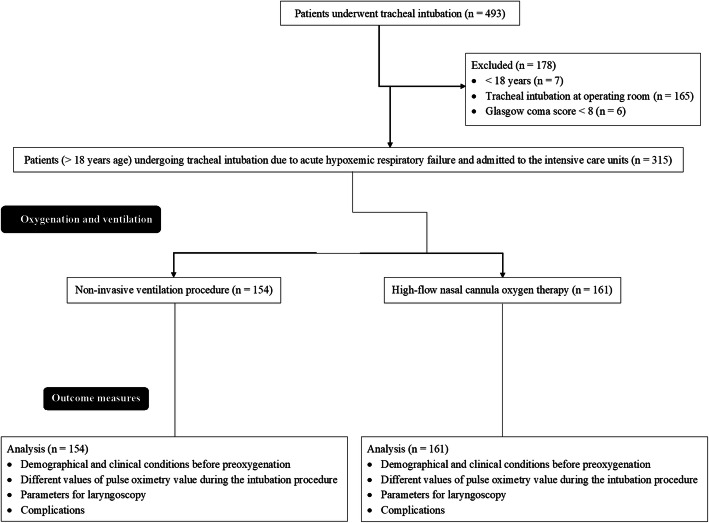
Patients underwent high-flow nasal cannula oxygen therapy (HCO cohort, n = 161) or non-invasive ventilation procedure (NIV cohort, n = 154) for oxygenation and ventilation due to acute hypoxemic respiratory failure in the intensive care unit. Data before preoxygenation, preoxygenation, intubation, laryngoscopy, and complications of patients due to tracheal intubation were retrospectively collected and analyzed.
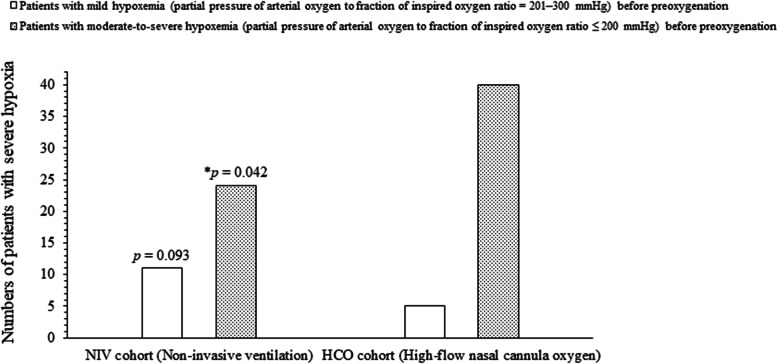
There was no difference between both cohorts for the demographical and clinical conditions of the patients before preoxygenation (p > 0.05 for all parameters), numbers of patients with severe hypoxia during the intubation procedure (35 vs. 45, p = 0.303), the time duration of laryngoscopy (p = 0.847), number of laryngoscopies attempts (p = 0.804), and immediate and late complications during the intubation procedure. The values of pulse oximetry were reported higher for patients of NIV cohort than those of HCO cohort during preoxygenation. Fewer numbers of patients were reported with severe hypoxia among patients of the NIV cohort than those of the HCO cohort (24 vs., 40, p = 0.042) who have moderate-to-severe hypoxemia (partial pressure of arterial oxygen to fraction of inspired oxygen ratio ≤ 200 mmHg) before preoxygenation. The most common complications were hypertension, pulmonary aspiration, and increased 30-day mortality.
When compared, there was no difference between non-invasive ventilation technique and high-flow oxygen therapy to minimize severe hypoxia prior to laryngoscopy and endotracheal intubation in patients with acute respiratory failure.
优化预充氧程序有助于通过降低严重低氧血症和其他问题的风险来确保插管方法的安全性。对于在插管过程中发生严重低氧血症的情况,与高流量氧疗相比,无创通气的效果存在混淆。本研究的目的是比较无创通气与高流量氧疗在预防喉镜检查期间缺氧方面的差异。
患者因急性低氧性呼吸衰竭在重症监护病房接受高流量鼻导管氧疗(HCO 队列,n=161)或无创通气程序(NIV 队列,n=154)进行氧合和通气。回顾性收集并分析患者在预充氧前、预充氧时、插管时、喉镜检查时以及因气管插管引起的并发症的数据。
在预充氧前,两组患者的人口统计学和临床状况无差异(所有参数的 p 值均>0.05),插管过程中严重缺氧的患者数量(35 例 vs. 45 例,p=0.303)、喉镜检查时间(p=0.847)、喉镜检查次数(p=0.804)以及插管过程中的即时和迟发性并发症均无差异。NIV 队列的患者在预充氧期间的脉搏血氧饱和度值报告高于 HCO 队列。在预充氧前有中重度低氧血症(动脉血氧分压与吸入氧分数比值≤200mmHg)的患者中,NIV 队列报告的严重缺氧患者数量少于 HCO 队列(24 例 vs. 40 例,p=0.042)。
与高流量氧疗相比,在急性呼吸衰竭患者中,进行无创通气技术与高流量氧疗以在喉镜检查和气管插管前最小化严重缺氧时,两者之间没有差异。