Kunder Viktor, Harris Johnathon, Moody Dyese
Internal Medicine, Brooke Army Medical Center, San Antonio, USA.
Cureus. 2025 May 8;17(5):e83752. doi: 10.7759/cureus.83752. eCollection 2025 May.
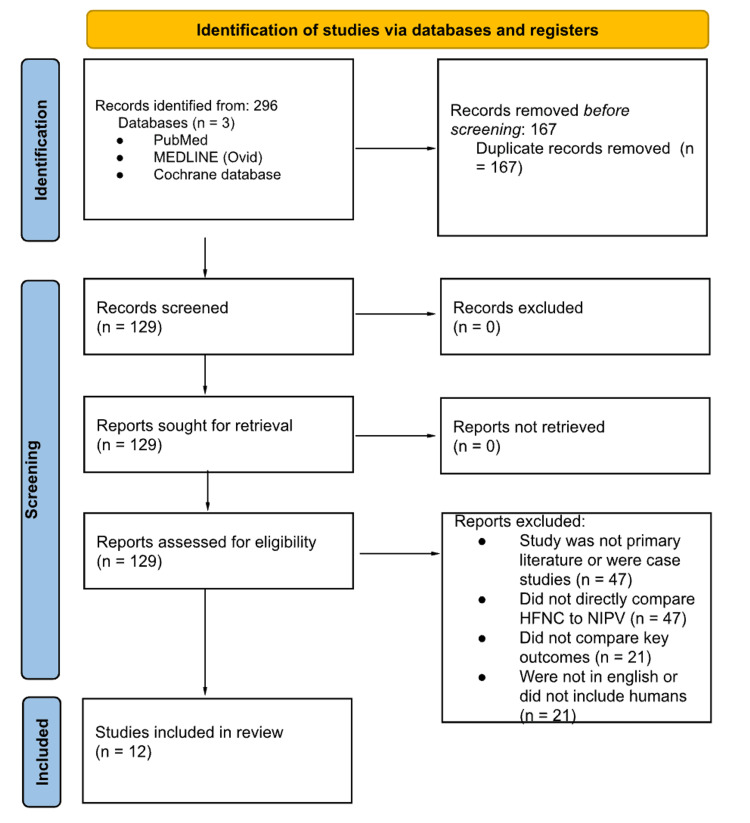
Acute hypoxemic respiratory failure (AHRF) is a leading cause of ICU admissions, and noninvasive respiratory support modalities such as high-flow nasal cannula (HFNC) and noninvasive ventilation (NIV) are frequently employed. However, the comparative effectiveness of these two interventions across different patient populations remains unclear. This scoping review aimed to synthesize current evidence comparing HFNC and NIV in the management of adult patients with AHRF, focusing on outcomes such as intubation rates, mortality, patient comfort, oxygenation, and complications. Studies were included if they: (1) were primary research articles, (2) involved human adults with AHRF, (3) directly compared HFNC with NIV, and (4) reported on clinical outcomes. Systematic reviews, case reports, editorials, and studies focused exclusively on immunocompromised or postoperative populations were excluded. A systematic search of PubMed, MEDLINE (via Ovid), and the Cochrane Library was conducted through February 2025. Three independent reviewers screened and selected studies using Rayyan. Data extraction was performed using a structured template capturing study design, sample size, population, intervention details, and relevant outcomes. Twelve studies met the inclusion criteria. HFNC and NIV demonstrated comparable effectiveness in reducing intubation rates across most patient populations. In COVID-19-associated AHRF, the two modalities yielded similar outcomes in terms of intubation and mortality. HFNC was consistently associated with greater patient comfort and fewer complications, particularly with respect to interface tolerance and skin breakdown. However, NIV remained more effective in clearing carbon dioxide, especially in patients with hypercapnic respiratory failure, such as those with COPD exacerbations. ORs were infrequently reported; however, one study reported an adjusted hazard ratio of 0.75 (95% CI: 0.58-0.98) favoring HFNC over oxygen masks for ICU mortality. HFNC may be preferable for patients who have difficulty tolerating masks or are at lower risk for hypercapnia, while NIV remains the standard of care in hypercapnic respiratory failure. Mortality outcomes were inconclusive. Future randomized controlled trials should target specific patient subgroups and examine long-term outcomes and hospital resource utilization to optimize noninvasive respiratory support strategies in AHRF.
急性低氧性呼吸衰竭(AHRF)是重症监护病房(ICU)收治患者的主要原因,高流量鼻导管(HFNC)和无创通气(NIV)等无创呼吸支持方式经常被采用。然而,这两种干预措施在不同患者群体中的相对有效性仍不明确。本综述旨在综合目前比较HFNC和NIV用于治疗成年AHRF患者的证据,重点关注插管率、死亡率、患者舒适度、氧合和并发症等结局。纳入的研究需满足以下条件:(1)为原始研究文章;(2)涉及患有AHRF的成年患者;(3)直接比较HFNC与NIV;(4)报告临床结局。排除系统评价、病例报告、社论以及专门针对免疫功能低下或术后人群的研究。通过2025年2月对PubMed、MEDLINE(通过Ovid)和Cochrane图书馆进行系统检索。三名独立评审员使用Rayyan筛选和选择研究。使用结构化模板进行数据提取,记录研究设计、样本量、人群、干预细节和相关结局。12项研究符合纳入标准。在大多数患者群体中,HFNC和NIV在降低插管率方面显示出相当的有效性。在与新型冠状病毒肺炎相关的AHRF中,这两种方式在插管和死亡率方面产生了相似的结局。HFNC始终与更高的患者舒适度和更少的并发症相关,特别是在接口耐受性和皮肤破损方面。然而,NIV在清除二氧化碳方面仍然更有效,尤其是在高碳酸血症性呼吸衰竭患者中,如慢性阻塞性肺疾病急性加重患者。很少有研究报告比值比(OR);然而,一项研究报告,与氧气面罩相比,HFNC降低ICU死亡率的调整后风险比为0.75(95%置信区间:0.58 - 0.98)。对于难以耐受面罩或高碳酸血症风险较低的患者,HFNC可能更可取,而NIV仍然是高碳酸血症性呼吸衰竭的标准治疗方法。死亡率结局尚无定论。未来的随机对照试验应针对特定患者亚组,并检查长期结局和医院资源利用情况,以优化AHRF的无创呼吸支持策略。