Department of Urology, Hirosaki University Graduate School of Medicine, Hirosaki, Japan.
Department of Glycotechnology, Center for Advanced Medical Research, Hirosaki University Graduate School of Medicine, Hirosaki, Japan.
Cancer Med. 2021 Feb;10(4):1297-1313. doi: 10.1002/cam4.3727. Epub 2021 Jan 16.
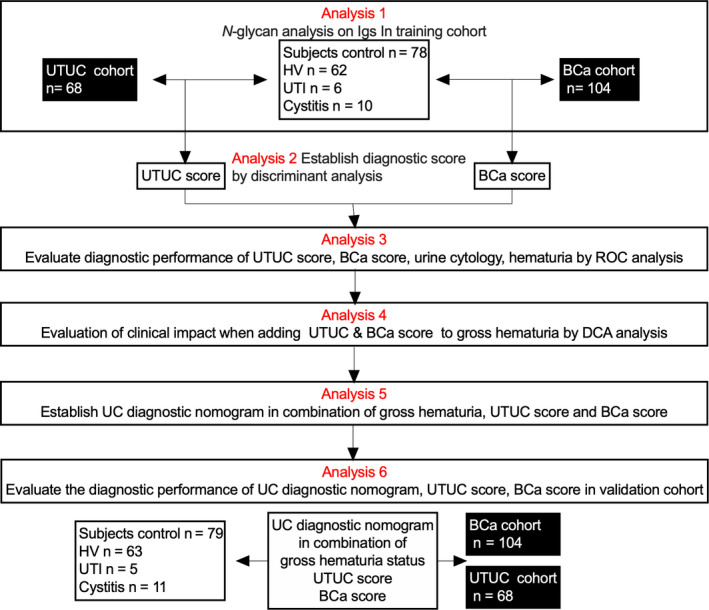
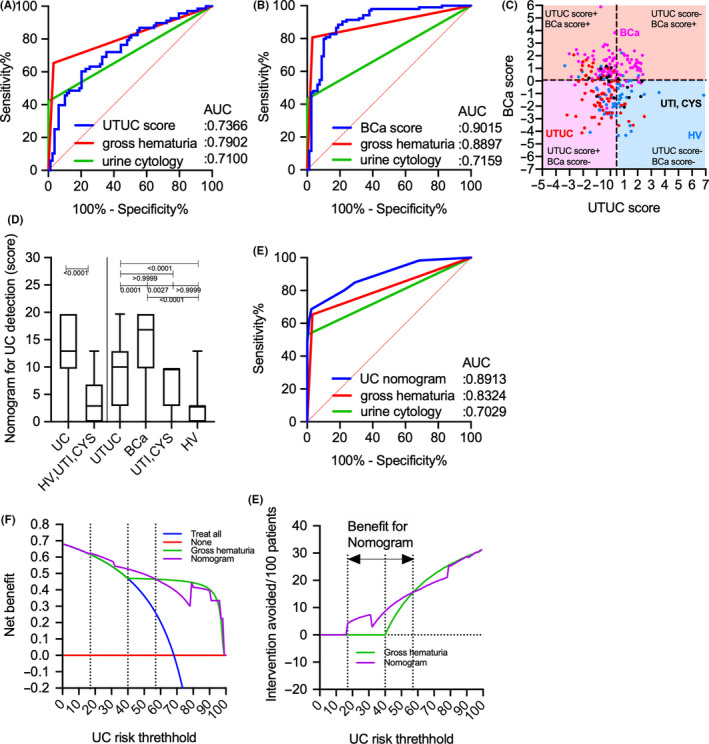
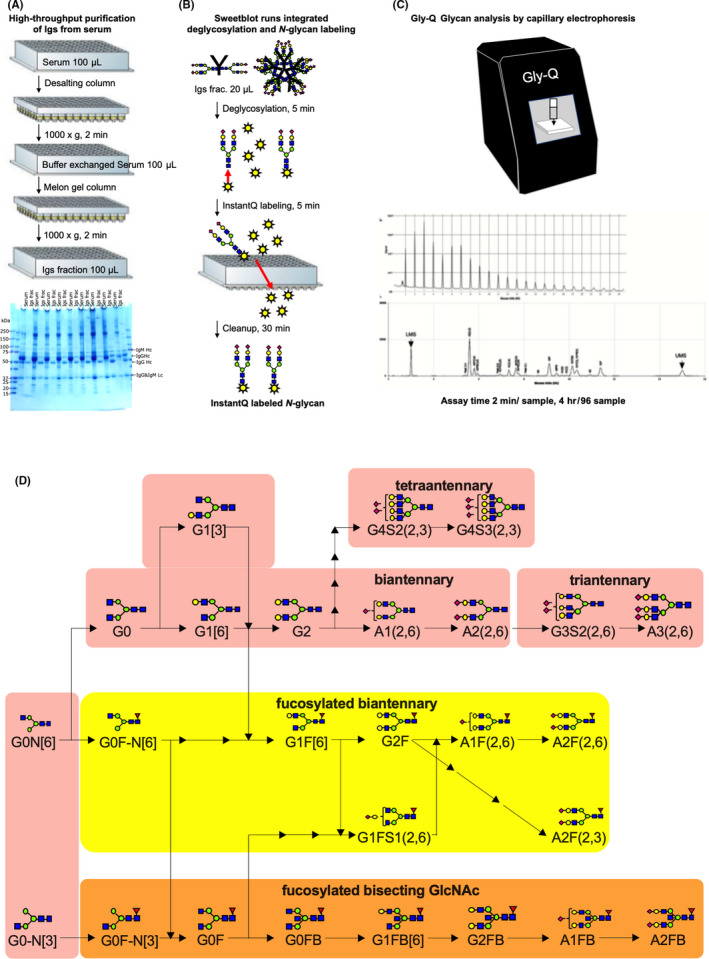
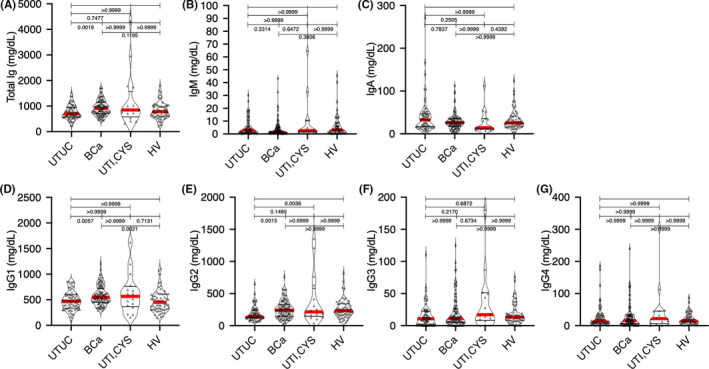
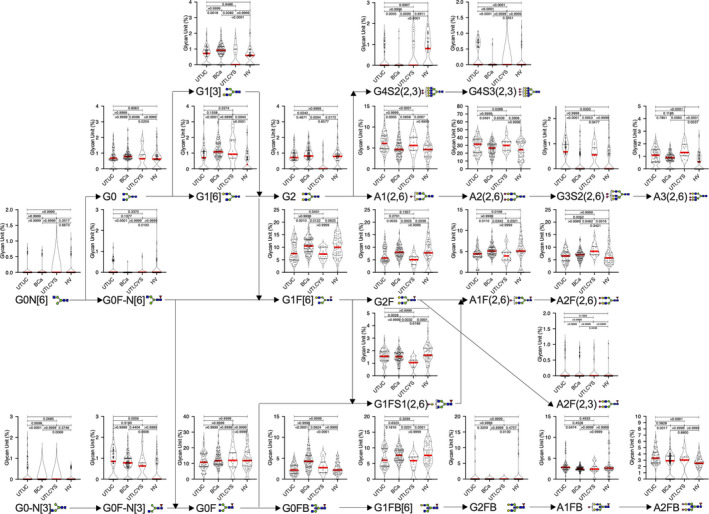
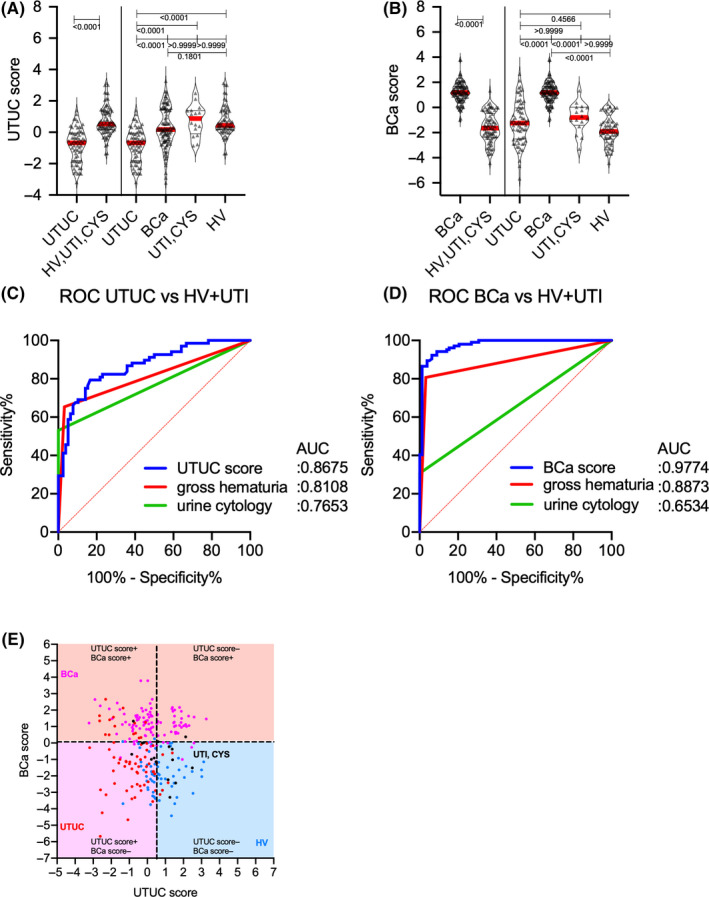
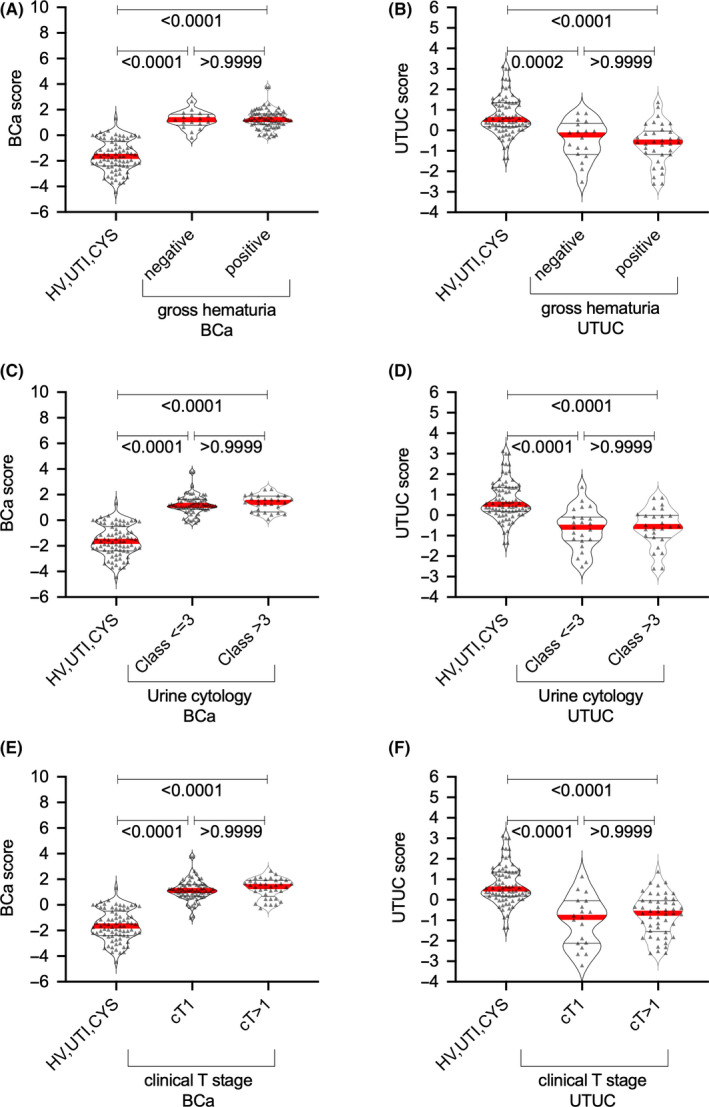
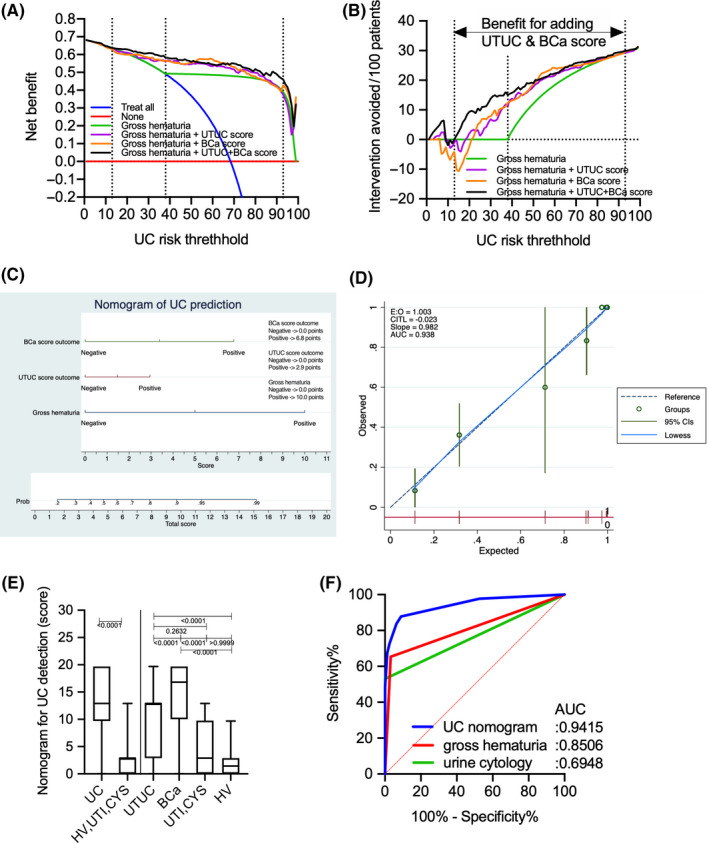
Discriminating between urothelial carcinoma (UC), including bladder cancer (BCa) and upper urinary tract UC (UTUC), is often challenging. Thus, the current study evaluated the diagnostic performance of N-glycosylation signatures of immunoglobulins (Igs) for detecting UC, including BCa and UTUC. N-glycosylation signatures of Igs from serum samples of the training cohort, including 104 BCa, 68 UTUC, 10 urinary tract infection, and 5 cystitis cases, as well as 62 healthy volunteers, were measured retrospectively using automated capillary-electrophoresis-based N-glycomics. UTUC or BCa scores were then established through discriminant analysis using N-glycan signatures of Igs. Diagnostic performance was evaluated using the area under receiver operating characteristics curve (AUC) and decision curve analyses (DCA). Our result showed that BCa and UTUC scores for discriminating BCa (AUC: 0.977) and UTUC (AUC: 0.867), respectively, provided significantly better clinical performance compared to urine cytology, gross hematuria, or clinical T1 cases. DCA revealed that adding BCa and UTUC scores to gross hematuria status was the best combination for detecting UC and avoiding the need for more intervention without overlooking UC (risk threshold: 13%-93%). The UC nomogram based on the combination of gross hematuria, UTUC score, and BCa score could detect UC with an AUC of 0.891, indicating significantly better performance compared to gross hematuria status in the validation cohort (251 patients). The limitations of this study include its small sample size and retrospective nature. The UC nomogram based on gross hematuria and N-glycosylation signatures of Igs can be a promising approach for the diagnosis of UC.
鉴别尿路上皮癌(UC),包括膀胱癌(BCa)和上尿路 UC(UTUC),通常具有挑战性。因此,本研究评估了免疫球蛋白(Ig)N-糖基化特征用于检测 UC,包括 BCa 和 UTUC 的诊断性能。使用基于自动毛细管电泳的 N-糖组学,回顾性测量了来自训练队列的血清样本中 Ig 的 N-糖基化特征,包括 104 例 BCa、68 例 UTUC、10 例尿路感染和 5 例膀胱炎病例以及 62 例健康志愿者。然后通过使用 Ig 的 N-聚糖特征进行判别分析来建立 UTUC 或 BCa 评分。使用接收者操作特征曲线(AUC)和决策曲线分析(DCA)评估诊断性能。结果表明,用于区分 BCa 的 BCa 和 UTUC 评分(AUC:0.977)和 UTUC(AUC:0.867),与尿细胞学、肉眼血尿或临床 T1 病例相比,提供了显著更好的临床性能。DCA 显示,将 BCa 和 UTUC 评分添加到肉眼血尿状态是检测 UC 并避免在不忽略 UC 的情况下需要更多干预的最佳组合(风险阈值:13%-93%)。基于肉眼血尿、UTUC 评分和 BCa 评分组合的 UC 列线图可检测到 UC,其 AUC 为 0.891,与验证队列中肉眼血尿状态相比,性能显著提高(251 例患者)。本研究的局限性包括样本量小和回顾性。基于肉眼血尿和 Ig N-糖基化特征的 UC 列线图可能是 UC 诊断的一种很有前途的方法。