Kalapara Arveen A, Frydenberg Mark
Department of Surgery, Monash University, Melbourne, Australia.
Cabrini Institute, Cabrini Health, Melbourne, Australia.
Transl Androl Urol. 2020 Dec;9(6):3123-3139. doi: 10.21037/tau-19-327.
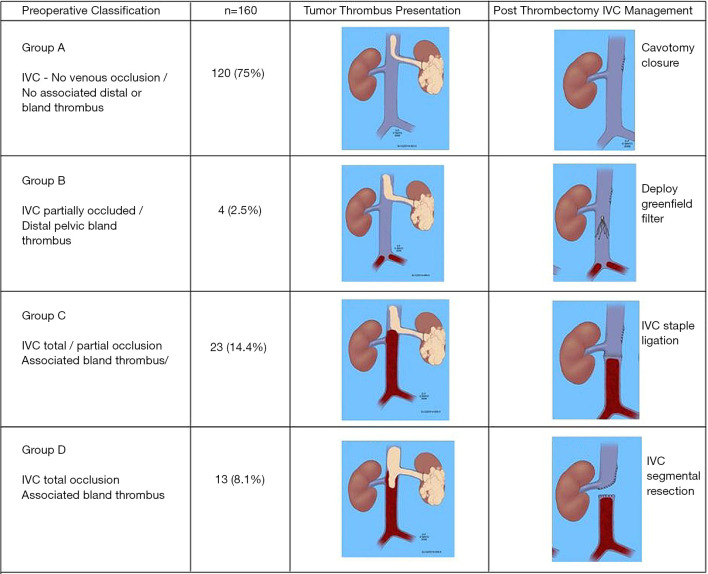
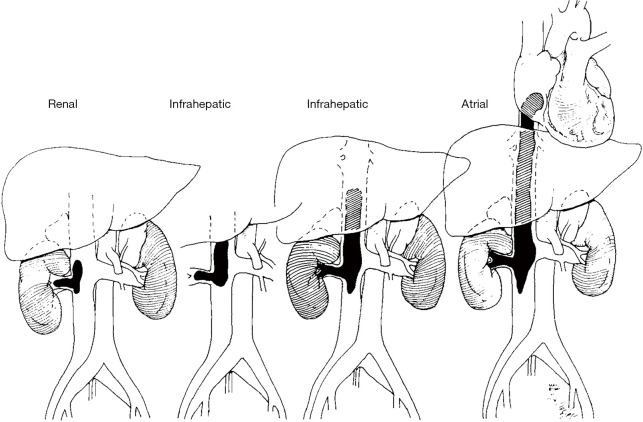
Radical nephrectomy (RN) remains a cornerstone of the management of localised renal cell carcinoma (RCC). RN involves the en bloc removal of the kidney along with perinephric fat enclosed within Gerota's fascia. Key principles of open RN include appropriate incision for adequate exposure, dissection and visualisation of the renal hilum, and early ligation of the renal artery and subsequently renal vein. Regional lymph node dissection (LND) facilitates local staging but its therapeutic role remains controversial. LND is recommended in patients with high risk clinically localised disease, but its benefit in low risk node-negative and clinically node-positive patients is unclear. Concomitant adrenalectomy should be reserved for patients with large tumours with radiographic evidence of adrenal involvement. Despite a recent downtrend in utilisation of open RN due to nephron-sparing and minimally invasive alternatives, there remains a vital role for open RN in the management of RCC in three domains. Firstly, open RN is important to the management of large, complex tumours which would be at high risk of complications if treated with partial nephrectomy (PN). Secondly, open RN plays a crucial role in cytoreductive nephrectomy (CN) for metastatic RCC, in which the laparoscopic approach achieves similar results but is associated with a high reoperation rate. Finally, open RN is the current standard of care in the management of inferior vena caval (IVC) tumour thrombus. Management of tumour thrombus requires a multidisciplinary approach and varies with cranial extent of thrombus. Higher level thrombus may require hepatic mobilisation and circulatory support, whilst the presence of bland thrombus may warrant post-operative filter insertion or ligation of the IVC.
根治性肾切除术(RN)仍然是局限性肾细胞癌(RCC)治疗的基石。RN包括整块切除肾脏以及肾周筋膜内的肾周脂肪。开放性RN的关键原则包括进行适当的切口以获得充分暴露、解剖和观察肾门,并早期结扎肾动脉,随后结扎肾静脉。区域淋巴结清扫术(LND)有助于局部分期,但其治疗作用仍存在争议。对于临床局限性高危疾病患者建议进行LND,但对于低风险淋巴结阴性和临床淋巴结阳性患者其益处尚不清楚。对于有影像学证据显示肾上腺受累的大肿瘤患者应保留肾上腺切除术。尽管由于保留肾单位和微创替代方案,开放性RN的应用最近呈下降趋势,但开放性RN在RCC治疗的三个领域中仍起着至关重要的作用。首先,开放性RN对于大的复杂肿瘤的治疗很重要,如果采用部分肾切除术(PN)治疗,这些肿瘤会有很高的并发症风险。其次,开放性RN在转移性RCC的减瘤性肾切除术(CN)中起着关键作用,在这种手术中,腹腔镜手术方法可取得类似结果,但再手术率较高。最后,开放性RN是目前治疗下腔静脉(IVC)肿瘤血栓的标准治疗方法。肿瘤血栓的治疗需要多学科方法,并且随血栓的头端范围而有所不同。较高水平的血栓可能需要肝脏游离和循环支持,而存在非感染性血栓可能需要术后置入滤网或结扎IVC。