Nguyen Cindy, Kortlever Joost T P, Gonzalez Amanda I, Ring David, Brown Laura E, Somogyi Jason R
Department of Surgery and Perioperative Care, Dell Medical School-The University of Texas at Austin, Austin, TX, USA.
Center for Health Communication, Dell Medical School-The University of Texas at Austin, Austin, TX, USA.
J Patient Exp. 2020 Dec;7(6):1094-1100. doi: 10.1177/2374373520930468. Epub 2020 Jun 11.
Measures of patient satisfaction are increasingly used to measure patient experience. Most satisfaction measures have notable ceiling effects, which limits our ability to learn from variation among relatively satisfied patients. This study tested a variety of single-question satisfaction measures for their mean overall score, ceiling and floor effect, and data distribution. In addition, we assessed the correlation between satisfaction and psychological factors and assessed how the various methods for measuring satisfaction affected net promoter scores (NPSs).
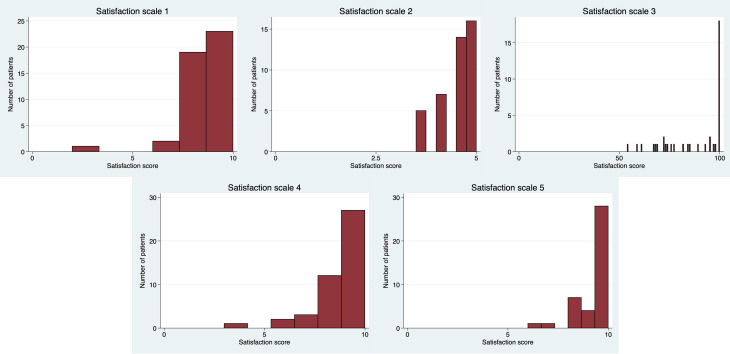
A total of 212 patients visiting orthopedic offices were enrolled in this randomized controlled trial. Patients were randomized to 1 of 5 newly designed, single-question satisfaction scales: (a) a helpfulness 11-point ordinal scale from 0 to 10, (b) a helpfulness ordinal 11-point scale from 0 to 5 (ie, with 1.5, 2.5, etc), (c) a helpfulness 100-point slider, (d) a satisfaction 11-point ordinal scale from 0 to 10, and (e) a willingness to recommend 11-point ordinal scale from 0 to 10. Additionally, patients completed the 2-item Pain Self-Efficacy Questionnaire (PSEQ-2), 5-item Short Health Anxiety Inventory (SHAI-5) Scale, and Patient-Reported Outcomes Measurement Information System (PROMIS) Depression. We assessed mean and median score, ceiling and floor effect, and skewness and kurtosis for each scale. Spearman's correlation tests were used to test correlations between satisfaction and psychological status. Finally, we assessed the NPS for the various scales.
Ceiling effects ranged from 29% to 68%. The 11-point ordinal helpfulness scale from 0 to 10 had the least ceiling effect (29%). All of the scales were asymmetrically distributed, with the 11-point ordinal scale from 0 to 5 having the most Gaussian distribution (skew = 0.64 and kurtosis = 2.3). Satisfaction scores did not correlate with psychological factors: PSEQ-2 ( = 0.04; = .57), SHAI-5 ( = 0.01; = .93), and PROMIS Depression ( = -0.04; = .61). Net promoter scores varied substantially by scale design, with higher scores corresponding with greater ceiling effects.
Variations in scale types, text anchors, and lead-in statements do not eliminate the ceiling effect of single-question measures of satisfaction with a visit to an orthopedic specialist. Further studies might test other scale designs and labels.
Diagnostic; Level II.
患者满意度测量方法越来越多地用于衡量患者体验。大多数满意度测量方法都有显著的天花板效应,这限制了我们从相对满意的患者之间的差异中学习的能力。本研究测试了多种单问题满意度测量方法的平均总分、天花板和地板效应以及数据分布。此外,我们评估了满意度与心理因素之间的相关性,并评估了各种满意度测量方法如何影响净推荐值(NPS)。
共有212名到骨科诊所就诊的患者参与了这项随机对照试验。患者被随机分配到5种新设计的单问题满意度量表中的一种:(a)一个从0到10的11点有序帮助程度量表,(b)一个从0到5的11点有序帮助程度量表(即有1.5、2.5等),(c)一个100点的帮助程度滑动量表,(d)一个从0到10的11点有序满意度量表,以及(e)一个从0到10的11点有序推荐意愿量表。此外,患者还完成了2项疼痛自我效能量表(PSEQ - 2)、5项简短健康焦虑量表(SHAI - 5)以及患者报告结局测量信息系统(PROMIS)抑郁量表。我们评估了每个量表的平均分和中位数、天花板和地板效应以及偏度和峰度。使用斯皮尔曼相关性检验来测试满意度与心理状态之间的相关性。最后,我们评估了各种量表的净推荐值。
天花板效应范围为29%至68%。从0到10的11点有序帮助程度量表的天花板效应最小(29%)。所有量表均呈非对称分布,从0到5的11点有序量表的高斯分布最明显(偏度 = 0.64,峰度 = 2.3)。满意度得分与心理因素不相关:PSEQ - 2(r = 0.04;p = 0.57)、SHAI - 5(r = 0.01;p = 0.93)和PROMIS抑郁量表(r = -0.04;p = 0.61)。净推荐值因量表设计而异,天花板效应越大得分越高。
量表类型、文本锚点和引导性陈述的变化并不能消除针对骨科专家就诊的单问题满意度测量的天花板效应。进一步的研究可能会测试其他量表设计和标签。
诊断性;二级。