Winter Johanna, Ellerbrock Malte, Jäkel Oliver, Greilich Steffen, Bangert Mark
Department of Medical Physics in Radiation Oncology, German Cancer Research Center (DKFZ), Im Neuenheimer Feld 280, 69120 Heidelberg, Germany.
Department of Physics and Astronomy, Heidelberg University, Heidelberg, Germany.
Phys Imaging Radiat Oncol. 2020 May 26;14:32-38. doi: 10.1016/j.phro.2020.05.001. eCollection 2020 Apr.
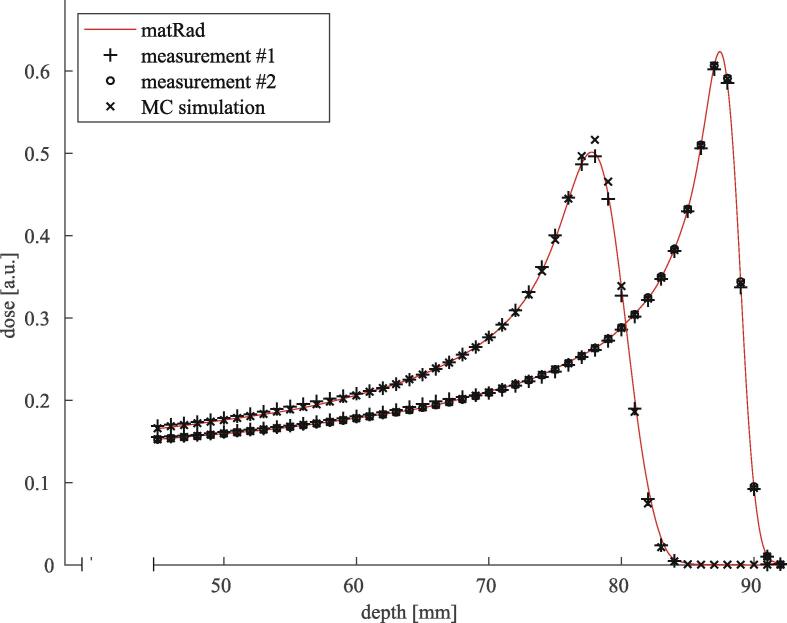
Proton therapy may be promising for treating non-small-cell lung cancer due to lower doses to the lung and heart, as compared to photon therapy. A reported challenge is degradation, , a smoothing of the depth-dose distribution due to heterogeneous lung tissue. For pencil beams, this causes a distal falloff widening and a peak-to-plateau ratio decrease, not considered in clinical treatment planning systems.
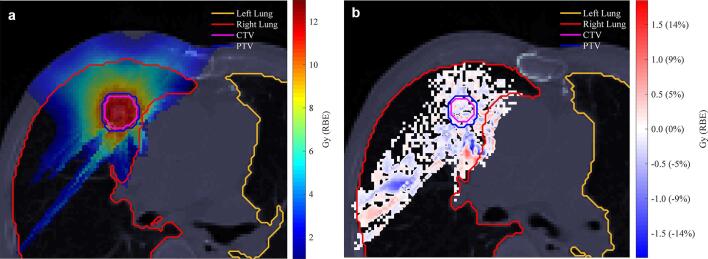
We present a degradation model implemented into an analytical dose calculation, fully integrated into a treatment planning workflow. Degradation effects were investigated on target dose, distal dose falloffs, and mean lung dose for ten patient cases with varying anatomical characteristics.
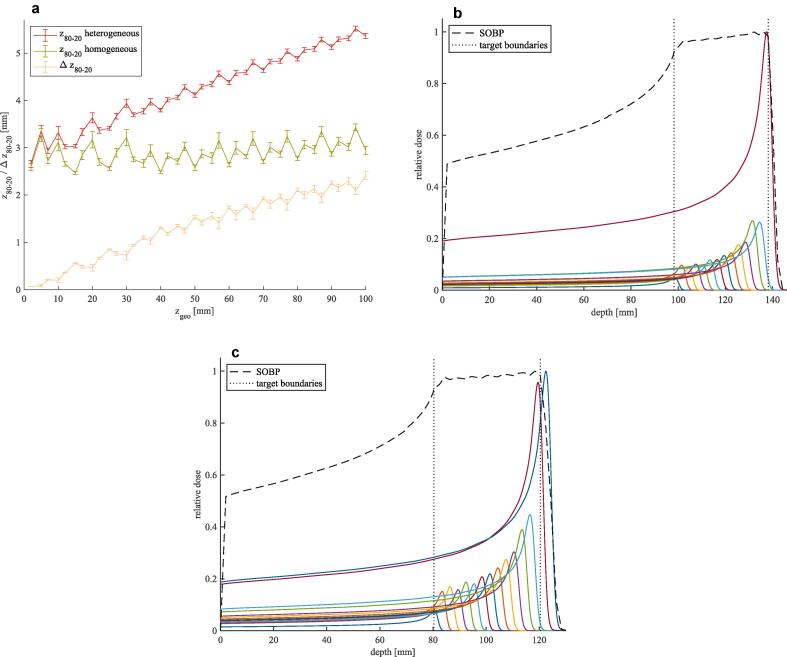
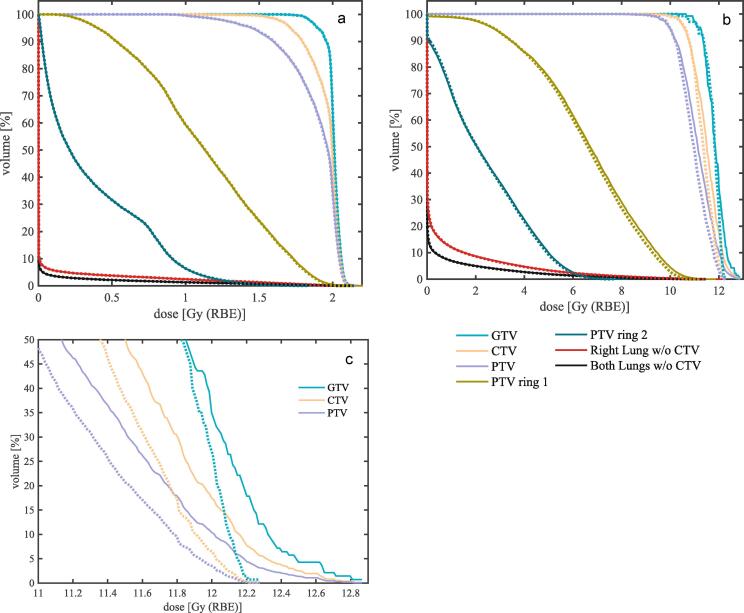
For patients with pronounced range straggling (in our study large tumors, or lesions close to the mediastinum), degradation effects were restricted to a maximum decrease in target coverage ( of the planning target volume) of 1.4%. The median broadening of the distal 80-20% dose falloffs was 0.5 mm at the maximum. For small target volumes deep inside lung tissue, however, the target underdose increased considerably by up to 26%. The mean lung dose was not negatively affected by degradation in any of the investigated cases.
For most cases, dose degradation due to heterogeneous lung tissue did not yield critical organ at risk overdosing or overall target underdosing. However, for small and deep-seated tumors which can only be reached by penetrating lung tissue, we have seen substantial local underdose, which deserves further investigation, also considering other prevalent sources of uncertainty.
与光子治疗相比,质子治疗对肺部和心脏的剂量较低,在治疗非小细胞肺癌方面可能具有前景。据报道,一个挑战是降解,即由于肺组织不均匀导致深度剂量分布平滑。对于笔形束,这会导致远端剂量下降变宽和峰谷比降低,而临床治疗计划系统中并未考虑这些因素。
我们提出了一种降解模型,该模型已应用于解析剂量计算中,并完全集成到治疗计划工作流程中。针对十例具有不同解剖特征患者的靶区剂量、远端剂量下降和平均肺剂量,研究了降解效应。
对于射程离散明显的患者(在我们的研究中为大肿瘤或靠近纵隔的病变),降解效应导致靶区覆盖度(计划靶体积的)最大降低1.4%。远端80 - 20%剂量下降的最大中位增宽为0.5毫米。然而,对于肺组织深处的小靶区体积,靶区剂量不足最多可显著增加26%。在任何研究病例中,平均肺剂量均未受到降解的负面影响。
在大多数情况下,肺组织不均匀导致的剂量降解不会使危及器官的剂量过量或总体靶区剂量不足。然而,对于只能通过穿透肺组织才能到达的小而深部的肿瘤,我们观察到了显著的局部剂量不足,这值得进一步研究,同时也应考虑其他常见的不确定性来源。