University of Pennsylvania Health System, Philadelphia, Pennsylvania (G.L.A., J.J., M.O.H., J.H.A., J.B., C.B., P.J.B., C.L.C., L.M.C., M.F.C., J.M.C., J.D.C., T.C., K.R.C., B.D.F., E.G., J.C.G., S.G., A.H., C.W.H., M.H., P.K., Z.N.K., G.B.K., M.L., N.D.M., M.E.M., D.N., J.L.P., M.B.P., S.C.P., Z.A.Q., J.P.R., J.S., W.D.S., M.J.S., M.G.S., C.P.S., J.K.W., W.W., A.A.W., B.J.A., J.T.G.).
Ann Intern Med. 2021 May;174(5):613-621. doi: 10.7326/M20-5327. Epub 2021 Jan 19.
The coronavirus disease 2019 (COVID-19) pandemic continues to surge in the United States and globally.
To describe the epidemiology of COVID-19-related critical illness, including trends in outcomes and care delivery.
Single-health system, multihospital retrospective cohort study.
5 hospitals within the University of Pennsylvania Health System.
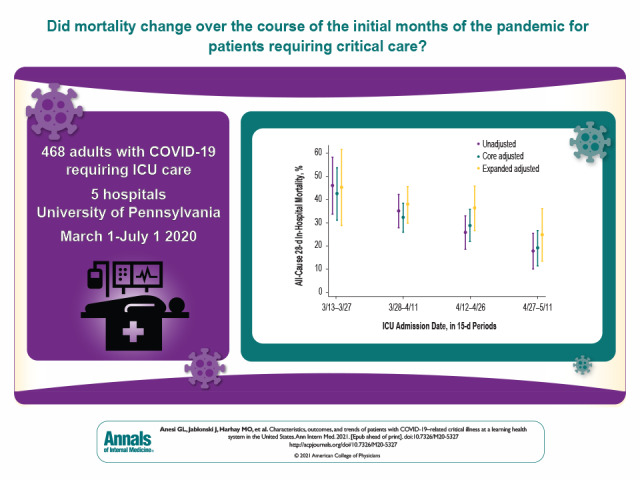
Adults with COVID-19-related critical illness who were admitted to an intensive care unit (ICU) with acute respiratory failure or shock during the initial surge of the pandemic.
The primary exposure for outcomes and care delivery trend analyses was longitudinal time during the pandemic. The primary outcome was all-cause 28-day in-hospital mortality. Secondary outcomes were all-cause death at any time, receipt of mechanical ventilation (MV), and readmissions.
Among 468 patients with COVID-19-related critical illness, 319 (68.2%) were treated with MV and 121 (25.9%) with vasopressors. Outcomes were notable for an all-cause 28-day in-hospital mortality rate of 29.9%, a median ICU stay of 8 days (interquartile range [IQR], 3 to 17 days), a median hospital stay of 13 days (IQR, 7 to 25 days), and an all-cause 30-day readmission rate (among nonhospice survivors) of 10.8%. Mortality decreased over time, from 43.5% (95% CI, 31.3% to 53.8%) to 19.2% (CI, 11.6% to 26.7%) between the first and last 15-day periods in the core adjusted model, whereas patient acuity and other factors did not change.
Single-health system study; use of, or highly dynamic trends in, other clinical interventions were not evaluated, nor were complications.
Among patients with COVID-19-related critical illness admitted to ICUs of a learning health system in the United States, mortality seemed to decrease over time despite stable patient characteristics. Further studies are necessary to confirm this result and to investigate causal mechanisms.
Agency for Healthcare Research and Quality.
2019 年冠状病毒病(COVID-19)大流行仍在美国和全球范围内持续蔓延。
描述 COVID-19 相关危重症的流行病学情况,包括结局和医疗护理提供趋势。
单医疗体系、多医院回顾性队列研究。
宾夕法尼亚大学卫生系统的 5 家医院。
COVID-19 相关危重症患者,这些患者在大流行初期因急性呼吸衰竭或休克而入住重症监护病房(ICU)。
结局和医疗护理提供趋势分析的主要暴露因素是大流行期间的纵向时间。主要结局为全因 28 天院内死亡率。次要结局为全因任何时间死亡率、接受机械通气(MV)和再入院。
在 468 例 COVID-19 相关危重症患者中,319 例(68.2%)接受 MV 治疗,121 例(25.9%)接受血管加压素治疗。结局包括全因 28 天院内死亡率为 29.9%、中位 ICU 住院时间为 8 天(四分位距 [IQR],3 至 17 天)、中位住院时间为 13 天(IQR,7 至 25 天)以及全因 30 天再入院率(非临终关怀幸存者)为 10.8%。在核心调整模型中,死亡率随时间逐渐下降,从第 1 个和最后 15 天期的 43.5%(95%CI,31.3%至 53.8%)降至 19.2%(CI,11.6%至 26.7%),而患者严重程度和其他因素并未改变。
单医疗体系研究;未评估其他临床干预措施的使用情况或其动态趋势,也未评估并发症。
在美国学习型医疗体系的 ICU 中收治的 COVID-19 相关危重症患者,尽管患者特征稳定,但死亡率似乎随时间逐渐下降。还需要进一步的研究来证实这一结果,并探讨因果机制。
美国医疗保健研究与质量署。