Papadimitriou-Olivgeris Matthaios, Bartzavali Christina, Georgakopoulou Alexandra, Kolonitsiou Fevronia, Papamichail Chrisavgi, Spiliopoulou Iris, Christofidou Myrto, Fligou Fotini, Marangos Markos
Division of Infectious Diseases, School of Medicine, University of Patras, 26504 Patras, Greece.
Department of Microbiology, School of Medicine, University of Patras, 26504 Patras, Greece.
Antibiotics (Basel). 2021 Jan 15;10(1):76. doi: 10.3390/antibiotics10010076.
The increased frequency of bacteraemias caused by pandrug-resistant (PDR-Kp) has significant implications. The aim of the present study was to identify predictors associated with mortality of PDR-Kp bacteraemias.
Patients with monomicrobial bacteraemia due to PDR-Kp were included. was considered PDR if it showed resistance to all available groups of antibiotics. Primary outcome was 30-day mortality. Minimum inhibitory concentrations (MICs) of meropenem, tigecycline, fosfomycin, and ceftazidime/avibactam were determined by Etest, whereas for colistin, the broth microdilution method was applied. , , , and genes were detected by PCR.
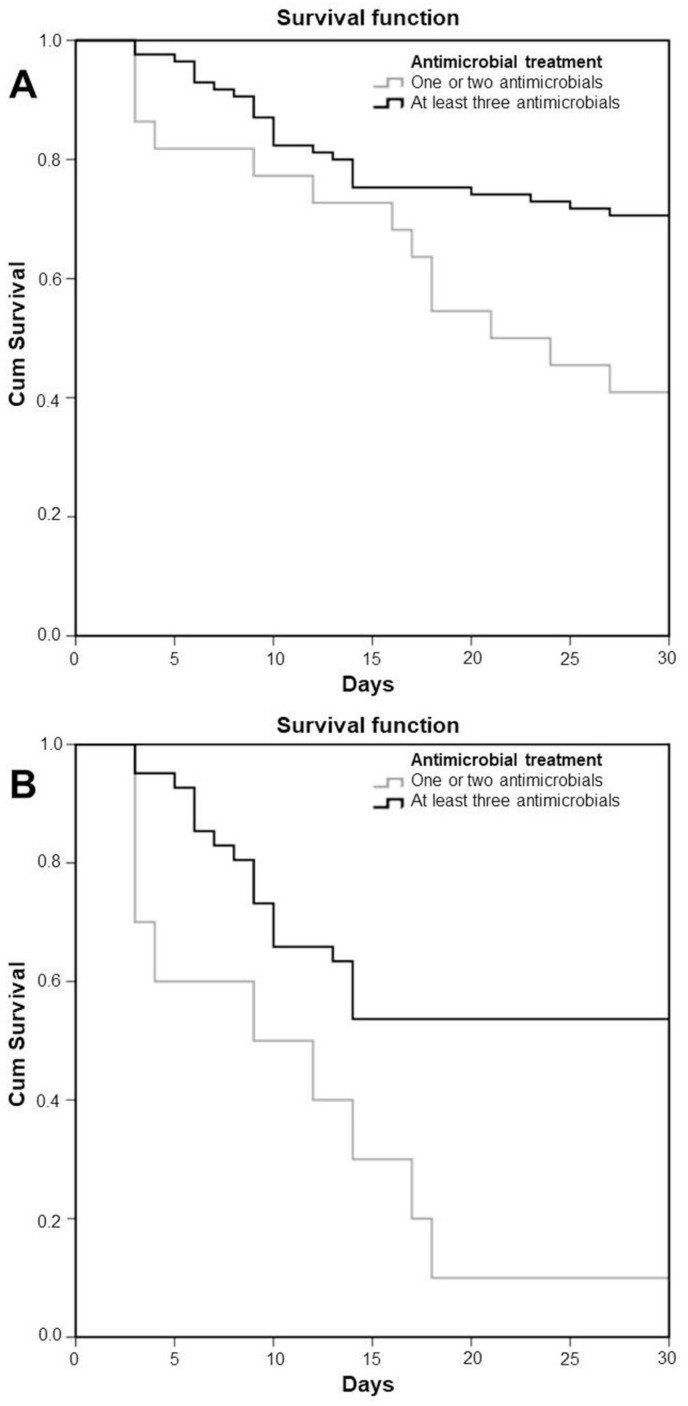
Among 115 PDR-Kp bacteraemias, the majority of infections were primary bacteraemias (53; 46.1%), followed by catheter-related (35; 30.4%). All isolates were resistant to tested antimicrobials. was the most prevalent carbapenemase gene (98 isolates; 85.2%). Thirty-day mortality was 39.1%; among 51 patients with septic shock, 30-day mortality was 54.9%. Multivariate analysis identified the development of septic shock, Charlson comorbidity index, and bacteraemia other than primary or catheter-related as independent predictors of mortality, while a combination of at least three antimicrobials was identified as an independent predictor of survival.
Mortality of PDR-Kp bloodstream infections was high. Administration of at least three antimicrobials might be beneficial for infections in critically ill patients caused by such pathogens.
泛耐药肺炎克雷伯菌(PDR-Kp)引起的菌血症频率增加具有重大影响。本研究的目的是确定与PDR-Kp菌血症死亡率相关的预测因素。
纳入因PDR-Kp引起的单微生物菌血症患者。如果对所有可用抗生素组均显示耐药,则被视为泛耐药。主要结局是30天死亡率。美罗培南、替加环素、磷霉素和头孢他啶/阿维巴坦的最低抑菌浓度(MIC)通过Etest测定,而对于黏菌素,则采用肉汤微量稀释法。通过PCR检测blaKPC、blaNDM、blaOXA-48和mcr-1基因。
在115例PDR-Kp菌血症中,大多数感染为原发性菌血症(53例;46.1%),其次是导管相关菌血症(35例;30.4%)。所有分离株均对测试抗菌药物耐药。blaKPC是最常见的碳青霉烯酶基因(98株;85.2%)。30天死亡率为39.1%;在51例感染性休克患者中,30天死亡率为54.9%。多变量分析确定感染性休克的发生、Charlson合并症指数以及非原发性或导管相关的菌血症是死亡率的独立预测因素,而至少三种抗菌药物联合使用是生存的独立预测因素。
PDR-Kp血流感染的死亡率很高。对于此类病原体引起的重症患者感染,使用至少三种抗菌药物可能有益。