1 Department of Medicine, Faculty of Medicine, The University of British Columbia, Vancouver, BC, Canada.
2 Penticton Regional Hospital Renal Program, Penticton, BC, Canada.
Palliat Med. 2018 Feb;32(2):395-403. doi: 10.1177/0269216317720832. Epub 2017 Jul 21.
End-stage kidney disease is associated with poor prognosis. Health care professionals must be prepared to address end-of-life issues and identify those at high risk for dying. A 6-month mortality prediction model for patients on dialysis derived in the United States is used but has not been externally validated.
We aimed to assess the external validity and clinical utility in an independent cohort in Canada.
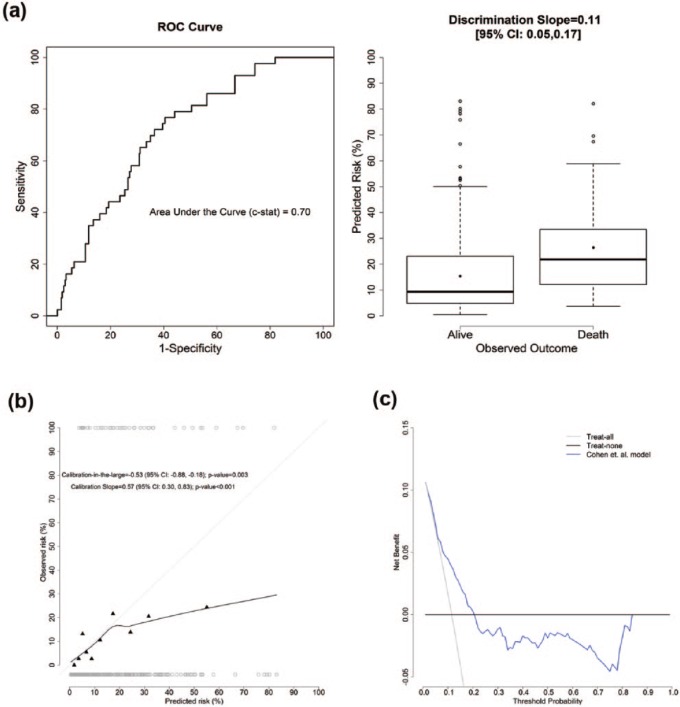
We examined the performance of the published 6-month mortality prediction model, using discrimination, calibration, and decision curve analyses.
SETTING/PARTICIPANTS: Data were derived from a cohort of 374 prevalent dialysis patients in two regions of British Columbia, Canada, which included serum albumin, age, peripheral vascular disease, dementia, and answers to the "the surprise question" ("Would I be surprised if this patient died within the next year?").
The observed mortality in the validation cohort was 11.5% at 6 months. The prediction model had reasonable discrimination (c-stat = 0.70) but poor calibration (calibration-in-the-large = -0.53 (95% confidence interval: -0.88, -0.18); calibration slope = 0.57 (95% confidence interval: 0.31, 0.83)) in our data. Decision curve analysis showed the model only has added value in guiding clinical decision in a small range of threshold probabilities: 8%-20%.
Despite reasonable discrimination, the prediction model has poor calibration in this external study cohort; thus, it may have limited clinical utility in settings outside of where it was derived. Decision curve analysis clarifies limitations in clinical utility not apparent by receiver operating characteristic curve analysis. This study highlights the importance of external validation of prediction models prior to routine use in clinical practice.
终末期肾病与预后不良相关。医疗保健专业人员必须准备好处理临终问题,并确定那些高风险死亡的患者。在美国开发的针对透析患者的 6 个月死亡率预测模型已经得到应用,但尚未经过外部验证。
我们旨在评估该模型在加拿大独立队列中的外部有效性和临床实用性。
我们使用判别分析、校准分析和决策曲线分析来评估已发表的 6 个月死亡率预测模型的性能。
设置/参与者:数据来自加拿大不列颠哥伦比亚省两个地区的 374 例透析患者队列,其中包括血清白蛋白、年龄、外周血管疾病、痴呆症以及对“意外问题”的回答(“如果这个患者在接下来的一年里去世,我会感到惊讶吗?”)。
验证队列中 6 个月的观察死亡率为 11.5%。该预测模型具有合理的判别能力(c 统计量=0.70),但校准不佳(大校准=-0.53(95%置信区间:-0.88,-0.18);校准斜率=0.57(95%置信区间:0.31,0.83))。决策曲线分析表明,该模型仅在阈值概率的小范围内(8%-20%)对指导临床决策具有附加价值。
尽管该预测模型具有合理的判别能力,但在该外部研究队列中校准不佳;因此,在模型来源之外的环境中,其临床实用性可能有限。决策曲线分析通过受试者工作特征曲线分析澄清了临床实用性的局限性。本研究强调了在常规临床实践中使用预测模型之前进行外部验证的重要性。