Fanizzi Annarita, Pomarico Domenico, Paradiso Angelo, Bove Samantha, Diotaiuti Sergio, Didonna Vittorio, Giotta Francesco, La Forgia Daniele, Latorre Agnese, Pastena Maria Irene, Tamborra Pasquale, Zito Alfredo, Lorusso Vito, Massafra Raffaella
Struttura Semplice Dipartimentale di Fisica Sanitaria, I.R.C.C.S. Istituto Tumori "Giovanni Paolo II", Viale Orazio Flacco 65, 70124 Bari, Italy.
Oncologia Medica Sperimentale, I.R.C.C.S. Istituto Tumori "Giovanni Paolo II", Viale Orazio Flacco 65, 70124 Bari, Italy.
Cancers (Basel). 2021 Jan 19;13(2):352. doi: 10.3390/cancers13020352.
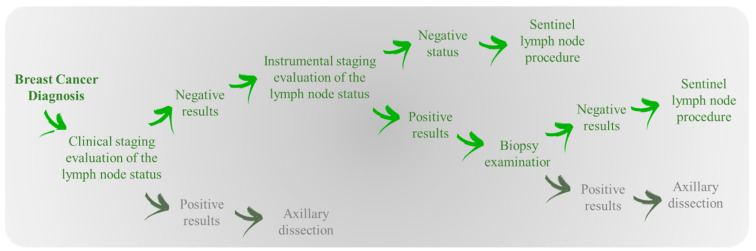
In the absence of lymph node abnormalities detectable on clinical examination or imaging, the guidelines provide for the dissection of the first axillary draining lymph nodes during surgery. It is not always possible to arrive at surgery without diagnostic doubts, and machine learning algorithms can support clinical decisions. The web calculator CancerMath (CM) allows you to estimate the probability of having positive lymph nodes valued on the basis of tumor size, age, histologic type, grading, expression of estrogen receptor, and progesterone receptor. We collected 993 patients referred to our institute with clinically negative results characterized by sentinel lymph node status, prognostic factors defined by CM, and also human epidermal growth factor receptor 2 (HER2) and Ki-67. Area Under the Curve (AUC) values obtained by the online CM application were comparable with those obtained after training its algorithm on our database. Nevertheless, by training the CM model on our dataset and using the same feature, we reached a sensitivity median value of 72%, whereas the online one was equal to 46%, despite a specificity reduction. We found that the addition of the prognostic factors Her2 and Ki67 could help improve performances on the classification of particular types of patients with the aim of reducing as much as possible the false positives that lead to axillary dissection. As showed by our experimental results, it is not particularly suitable for use as a support instrument for the prediction of metastatic lymph nodes on clinically negative patients.
若临床检查或影像学检查未发现淋巴结异常,指南规定手术时需清扫腋窝首站引流淋巴结。手术时并非总能毫无诊断疑虑,机器学习算法可为临床决策提供支持。网络计算器CancerMath(CM)可根据肿瘤大小、年龄、组织学类型、分级、雌激素受体和孕激素受体表达情况,估算淋巴结转移阳性的概率。我们收集了993例转诊至我院的患者资料,这些患者临床检查结果为阴性,记录了前哨淋巴结状态、CM定义的预后因素,以及人表皮生长因子受体2(HER2)和Ki-67情况。在线CM应用程序获得的曲线下面积(AUC)值与在我们的数据库上训练其算法后获得的值相当。然而,通过在我们的数据集中训练CM模型并使用相同特征,我们得到的敏感性中位数为72%,而在线模型为46%,尽管特异性有所降低。我们发现,添加预后因素Her2和Ki67有助于提高特定类型患者分类的性能,以尽可能减少导致腋窝清扫的假阳性结果。正如我们的实验结果所示,它不太适合用作临床阴性患者转移性淋巴结预测的辅助工具。