Department of Cardiovascular Medicine, Oakland University William Beaumont School of Medicine and Beaumont Hospital, Royal Oak, Michigan, USA.
Mediana Inc., Medford, Massachusetts, USA.
JACC Clin Electrophysiol. 2021 Jan;7(1):16-25. doi: 10.1016/j.jacep.2020.07.016. Epub 2020 Aug 5.
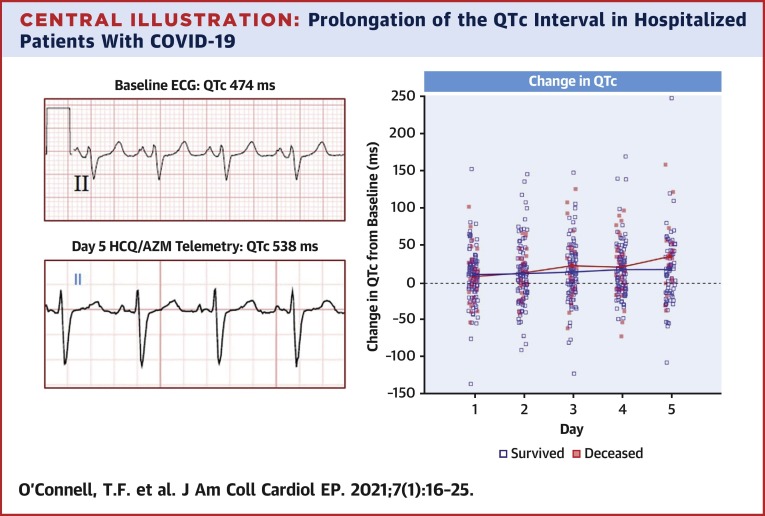
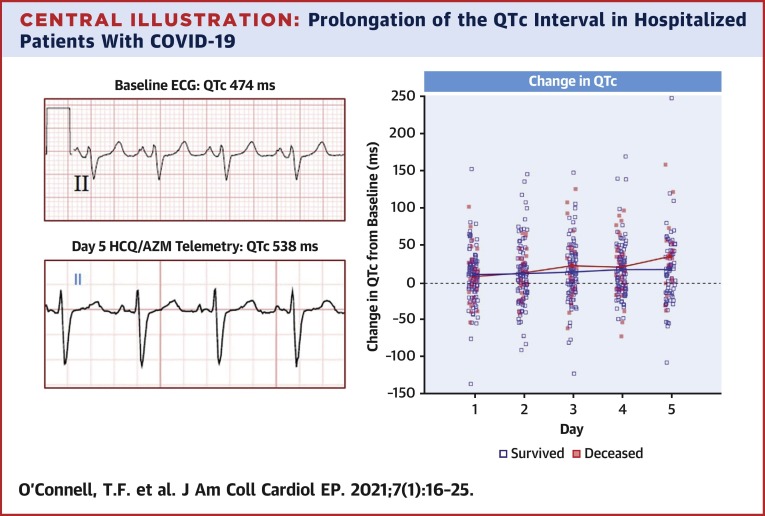
This study aimed to characterize corrected QT (QTc) prolongation in a cohort of hospitalized patients with coronavirus disease-2019 (COVID-19) who were treated with hydroxychloroquine and azithromycin (HCQ/AZM).
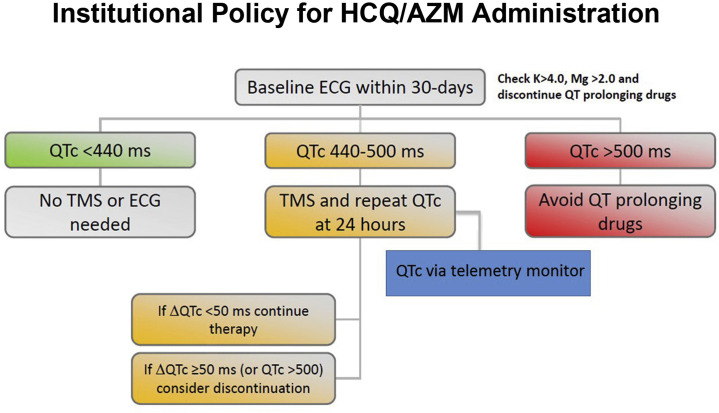
HCQ/AZM is being widely used to treat COVID-19 despite the known risk of QT interval prolongation and the unknown risk of arrhythmogenesis in this population.
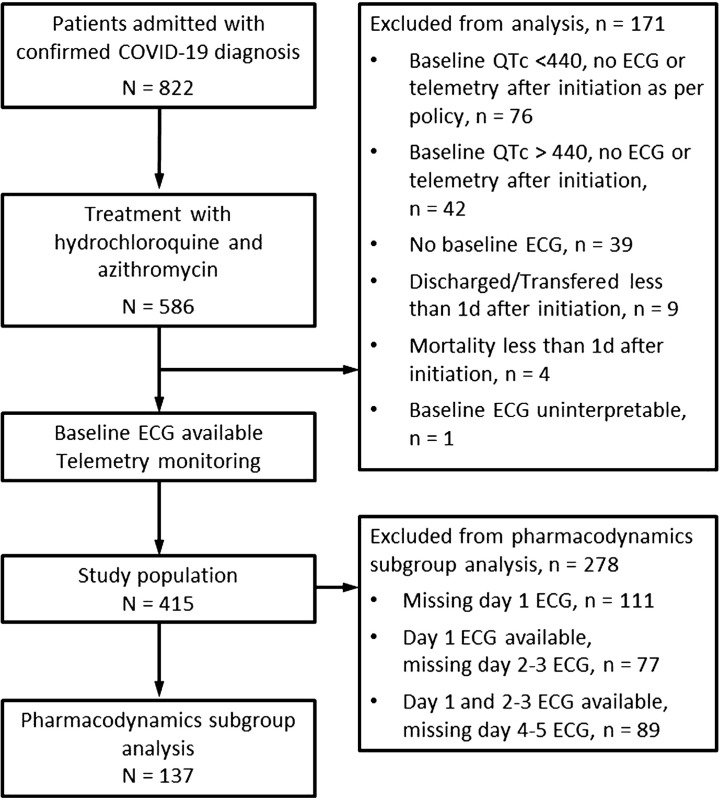
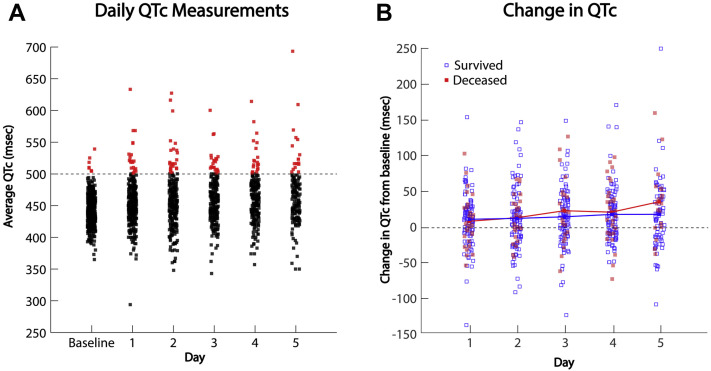
A retrospective cohort of COVID-19 hospitalized patients treated with HCQ/AZM was reviewed. The QTc interval was calculated before drug administration and for the first 5 days following initiation. The primary endpoint was the magnitude of QTc prolongation, and factors associated with QTc prolongation. Secondary endpoints were incidences of sustained ventricular tachycardia or ventricular fibrillation and all-cause mortality.
Among 415 patients who received concomitant HCQ/AZM, the mean QTc increased from 443 ± 25 ms to a maximum of 473 ± 40 ms (87 [21%] patients had a QTc ≥500 ms). Factors associated with QTc prolongation ≥500 ms were age (p < 0.001), body mass index <30 kg/m (p = 0.005), heart failure (p < 0.001), elevated creatinine (p = 0.005), and peak troponin (p < 0.001). The change in QTc was not associated with death over the short period of the study in a population in which mortality was already high (hazard ratio: 0.998; p = 0.607). No primary high-grade ventricular arrhythmias were observed.
An increase in QTc was seen in hospitalized patients with COVID-19 treated with HCQ/AZM. Several clinical factors were associated with greater QTc prolongation. Changes in QTc were not associated with increased risk of death.
本研究旨在描述住院的新型冠状病毒病 2019(COVID-19)患者接受羟氯喹和阿奇霉素(HCQ/AZM)治疗后的校正 QT(QTc)延长情况。
尽管已知 HCQ/AZM 会导致 QT 间期延长,并且该人群发生心律失常的风险未知,但仍广泛用于治疗 COVID-19。
回顾性分析了接受 HCQ/AZM 治疗的 COVID-19 住院患者队列。在给药前和起始后 5 天内计算 QTc 间期。主要终点是 QTc 延长的幅度以及与 QTc 延长相关的因素。次要终点为持续性室性心动过速或心室颤动的发生率和全因死亡率。
在接受 HCQ/AZM 联合治疗的 415 例患者中,平均 QTc 从 443±25ms 增加至最大值 473±40ms(87[21%]例患者的 QTc≥500ms)。与 QTc 延长≥500ms 相关的因素为年龄(p<0.001)、体重指数<30kg/m²(p=0.005)、心力衰竭(p<0.001)、肌酐升高(p=0.005)和肌钙蛋白峰值升高(p<0.001)。在死亡率已经很高的研究人群中,在短期研究期间,QTc 的变化与死亡无关(风险比:0.998;p=0.607)。未观察到原发性高级别室性心律失常。
接受 HCQ/AZM 治疗的 COVID-19 住院患者的 QTc 增加。几个临床因素与更大的 QTc 延长相关。QTc 的变化与死亡风险的增加无关。