Department of Cardiology, Angiology and Pulmonology, University Hospital Heidelberg, INF 410, 69120, Heidelberg, Germany.
Department of Radiation Oncology, Heidelberg Ion-Beam Therapy Center (HIT), German Cancer Research Center, Heidelberg University Hospital (UKHD), Heidelberg, Germany.
Clin Res Cardiol. 2021 Apr;110(4):579-590. doi: 10.1007/s00392-020-01801-y. Epub 2021 Jan 22.
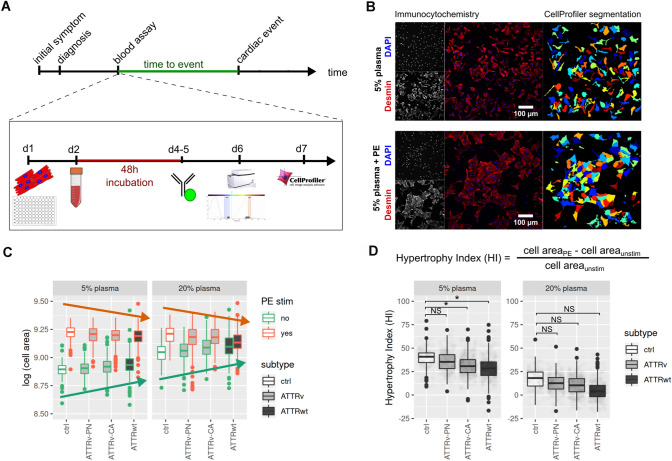
Direct toxic effects of transthyretin amyloid in patient plasma upon cardiomyocytes are discussed. However, no data regarding the relevance of this putative effect for clinical outcome are available. In this monocentric prospective study, we analyzed cellular hypertrophy after phenylephrine stimulation in vitro in the presence of patient plasma and correlated the cellular growth response with phenotype and prognosis.
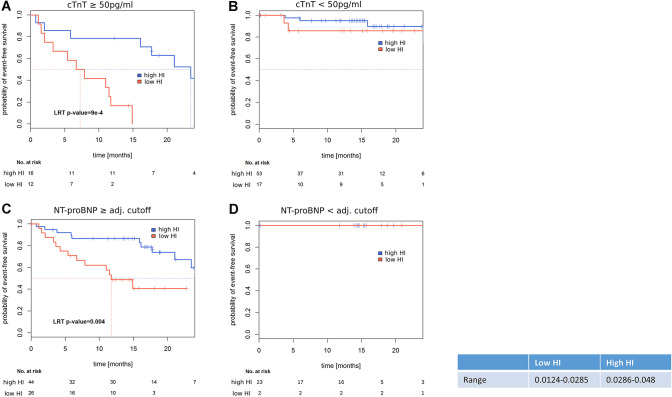
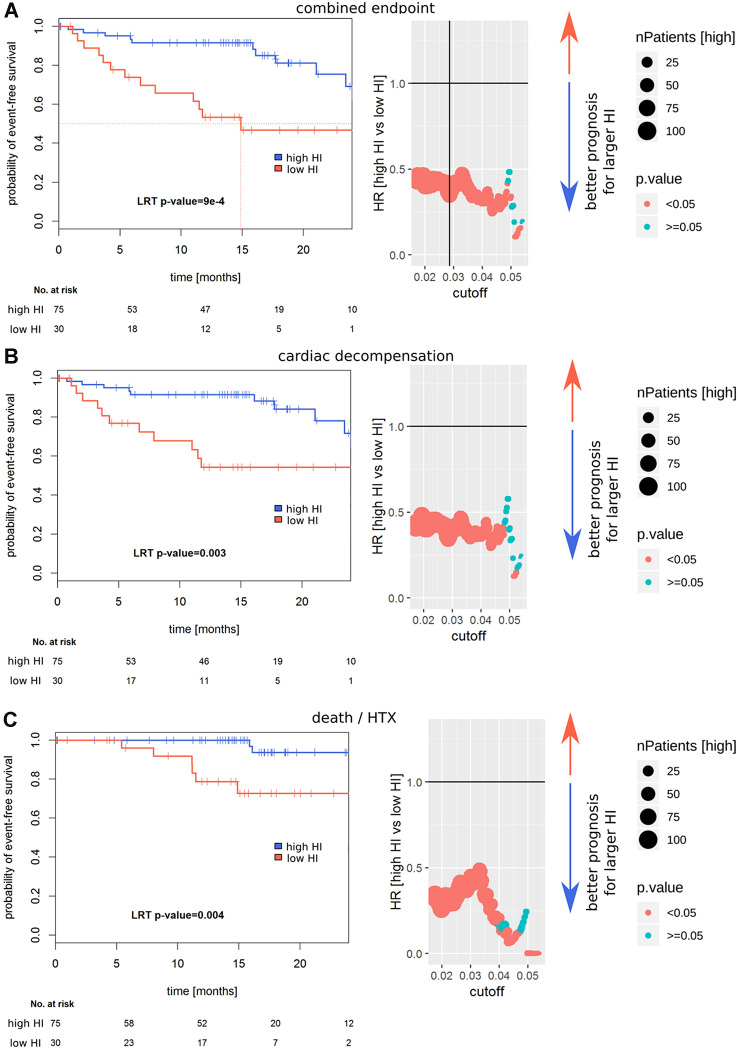
Progress in automated microscopy and image analysis allows high-throughput analysis of cell morphology. Using the InCell microscopy system, changes in cardiomyocyte's size after treatment with patient plasma from 89 patients suffering from transthyretin amyloidosis and 16 controls were quantified. For this purpose, we propose a novel metric that we named Hypertrophic Index, defined as difference in cell size after phenylephrine stimulation normalized to the unstimulated cell size. Its prognostic value was assessed for multiple endpoints (HTX: death/heart transplantation; DMP: cardiac decompensation; MACE: combined) using Cox proportional hazard models. Cells treated with plasma from healthy controls and hereditary transthyretin amyloidosis with polyneuropathy showed an increase in Hypertrophic Index after phenylephrine stimulation, whereas stimulation after treatment with hereditary cardiac amyloidosis or wild-type transthyretin patient plasma showed a significantly attenuated response. Hypertrophic Index was associated in univariate analyses with HTX (hazard ratio (HR) high vs low: 0.12 [0.02-0.58], p = 0.004), DMP: (HR 0.26 [0.11-0.62], p = 0.003) and MACE (HR 0.24 [0.11-0.55], p < 0.001). Its prognostic value was independent of established risk factors, cardiac TroponinT or N-terminal prohormone brain natriuretic peptide (NTproBNP).
Attenuated cardiomyocyte growth response after stimulation with patient plasma in vitro is an independent risk factor for adverse cardiac events in ATTR patients.
讨论转甲状腺素蛋白淀粉样变患者血浆对心肌细胞的直接毒性作用。然而,目前尚无关于这种推测的效应与临床结果相关性的数据。在这项单中心前瞻性研究中,我们分析了体外在患者血浆存在的情况下,苯肾上腺素刺激后心肌细胞的细胞肥大,并将细胞生长反应与表型和预后相关联。
自动化显微镜和图像分析的进展允许对细胞形态进行高通量分析。使用 InCell 显微镜系统,定量分析了 89 名转甲状腺素蛋白淀粉样变患者和 16 名对照患者的血浆处理后心肌细胞大小的变化。为此,我们提出了一种新的指标,我们称之为肥大指数,定义为苯肾上腺素刺激后细胞大小的差异与未刺激细胞大小的归一化。使用 Cox 比例风险模型评估其对多个终点(HTX:死亡/心脏移植;DMP:心脏失代偿;MACE:复合)的预后价值。用来自健康对照者和遗传性转甲状腺素蛋白淀粉样变伴多发性神经病患者的血浆处理的细胞在苯肾上腺素刺激后显示出肥大指数的增加,而用遗传性心脏淀粉样变或野生型转甲状腺素蛋白患者的血浆处理后刺激则显示出明显减弱的反应。在单变量分析中,肥大指数与 HTX 相关(高 vs 低 HR:0.12[0.02-0.58],p=0.004)、DMP(HR 0.26[0.11-0.62],p=0.003)和 MACE(HR 0.24[0.11-0.55],p<0.001)。其预后价值独立于已建立的危险因素、心肌肌钙蛋白 T 或 N 端前脑利钠肽(NTproBNP)。
体外用患者血浆刺激后心肌细胞生长反应减弱是 ATTR 患者不良心脏事件的独立危险因素。