Chung Doo Yong, Kang Dong Hyuk, Kim Jong Won, Kim Do Kyung, Lee Joo Yong, Cho Kang Su
Department of Urology, Inha University School of Medicine, Incheon, Korea.
Department of Urology, Gangnam Severance Hospital, Yonsei University College of Medicine, Gangnam-gu, Seoul, Korea.
Ther Adv Urol. 2020 Dec 25;12:1756287220981508. doi: 10.1177/1756287220981508. eCollection 2020 Jan-Dec.
Owing to the limited ability of current imaging modalities, several clinical T1 renal cell carcinomas (cT1 RCCa) can be pathologically upstaged to T3a (pT3a) after surgery. There have been some controversies regarding the oncological safety of partial nephrectomy (PNx) compared with radical nephrectomy (RNx) in these patients. We compared oncological outcomes of PNx and RNx in patients with upstaged pT3a RCCa.
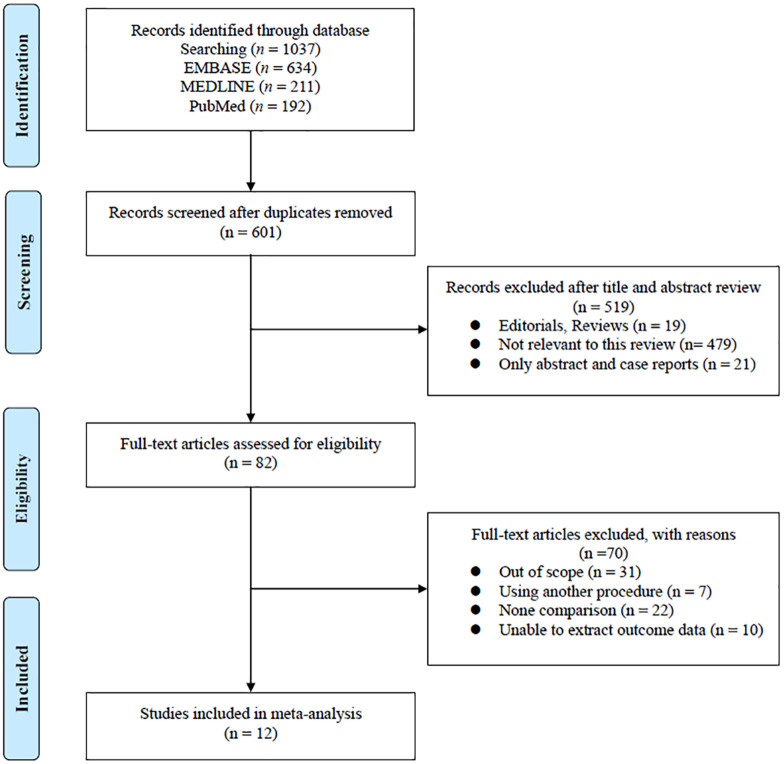
A systematic review was performed following the PRISMA guideline. PubMed, MEDLINE, Embase were searched. Oncological outcomes [recurrence-free survival (RFS), overall survival (OS) and cancer-specific survival (CSS)] between PNx and RNx were compared. The GRADE approach was used to rate the certainty of evidence.
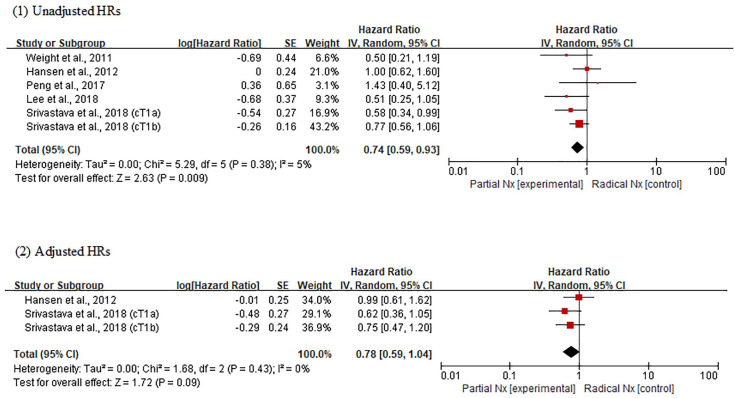
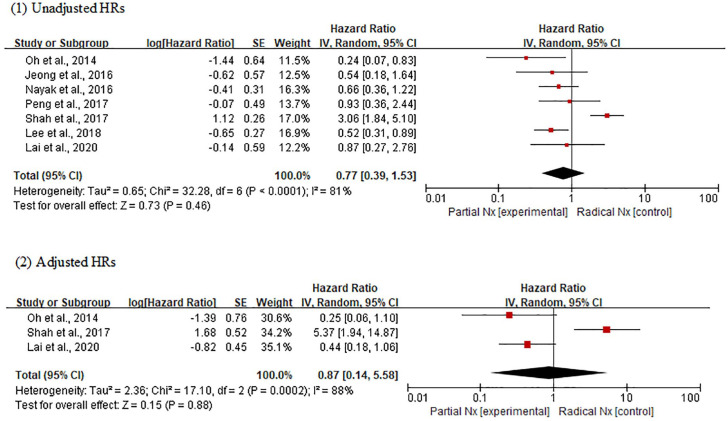
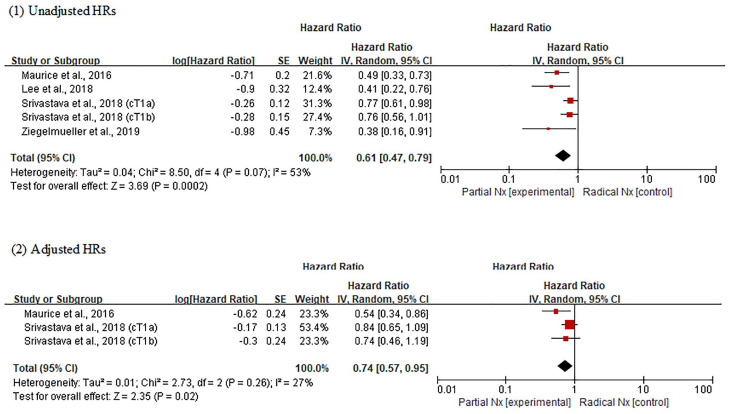
A total of 7406 patients in 12 articles related to upstaged pT3a RCCa were included. In adjusted analysis, no difference was observed in RFS [hazard ratios (HR) 0.87; 95% confidence intervals (CI), 0.57-0.95; = 0.88] and CSS (HR, 0.78; 95% CI, 0.59-1.04; = 0.09) for PNx and RNx. Meanwhile, PNx was significantly associated with favorable OS compared with RNx (HR, 0.74; 95% CI, 0.57-0.95; = 0.02).
Our meta-analysis shows that patients treated with PNx have better or at least similar oncological outcomes compared with RNx in patients with upstaged pT3a RCCa from cT1. In particular, patients who had undergone PNx show a significantly improved OS. If PNx is available, we recommend performing PNx for all cT1 RCCa, even in patients with upstaging potential. However, due to the low level of evidence, large-scale randomized trials are required.
由于当前成像方式的能力有限,一些临床T1期肾细胞癌(cT1 RCCa)在手术后病理分期可能会升至T3a(pT3a)。在这些患者中,与根治性肾切除术(RNx)相比,部分肾切除术(PNx)的肿瘤学安全性存在一些争议。我们比较了pT3a期肾细胞癌患者行PNx和RNx后的肿瘤学结局。
按照PRISMA指南进行系统评价。检索了PubMed、MEDLINE、Embase。比较了PNx和RNx之间的肿瘤学结局[无复发生存期(RFS)、总生存期(OS)和癌症特异性生存期(CSS)]。采用GRADE方法对证据的确定性进行评级。
共纳入12篇与pT3a期肾细胞癌相关文章中的7406例患者。在调整分析中,PNx和RNx的RFS[风险比(HR)0.87;95%置信区间(CI),0.57 - 0.95;P = 0.88]和CSS(HR,0.78;95%CI,0.59 - 1.04;P = 0.09)无差异。同时,与RNx相比,PNx与更好的OS显著相关(HR = 0.74;95%CI,0.57 - 0.95;P = 0.02)。
我们的荟萃分析表明,对于cT1期pT3a期肾细胞癌患者,与RNx相比,接受PNx治疗的患者具有更好或至少相似的肿瘤学结局。特别是,接受PNx的患者OS有显著改善。如果可以进行PNx,我们建议对所有cT1 RCCa患者进行PNx,即使是有分期上升可能的患者。然而,由于证据水平较低,需要进行大规模随机试验。