Ledermann Katharina, von Känel Roland, Barth Jürgen, Schnyder Ulrich, Znoj Hansjörg, Schmid Jean-Paul, Meister Langraff Rebecca E, Princip Mary
Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, University Hospital Zurich, and University of Zurich, Zurich, Switzerland.
Department of Clinical and Health Psychology, University of Fribourg, Fribourg, Switzerland.
Eur J Psychotraumatol. 2020 Sep 4;11(1):1804119. doi: 10.1080/20008198.2020.1804119.
It has been acknowledged that medical life-threatening experiences such as an acute myocardial infarction (MI) often lead to acute stress disorder symptoms (ASS), which in turn can result in the development of post-traumatic stress symptoms (PTSS). Previous studies have suggested an association between various traumatic experiences and alexithymia. The association of alexithymia with ASS and PTSS in patients with MI is elusive.
The aim of this study was to examine the association of alexithymia with MI-induced ASS and PTSS in patients at high risk of developing PTSD.
Patients ( = 154) were examined twice, once within 48 hours, and then again three months after acute MI. All patients completed the self-rating Acute Stress Disorder Scale (ASDS) within 48 hours after the cardiac event. Three months after hospital discharge, all patients completed the Toronto Alexithymia Scale (TAS-20) and underwent the Clinician-Administered PTSD Scale (CAPS), a structured interview to assess the severity of PTSS. Descriptive statistics, correlations, multivariate linear regressions, and moderation analysis were conducted.
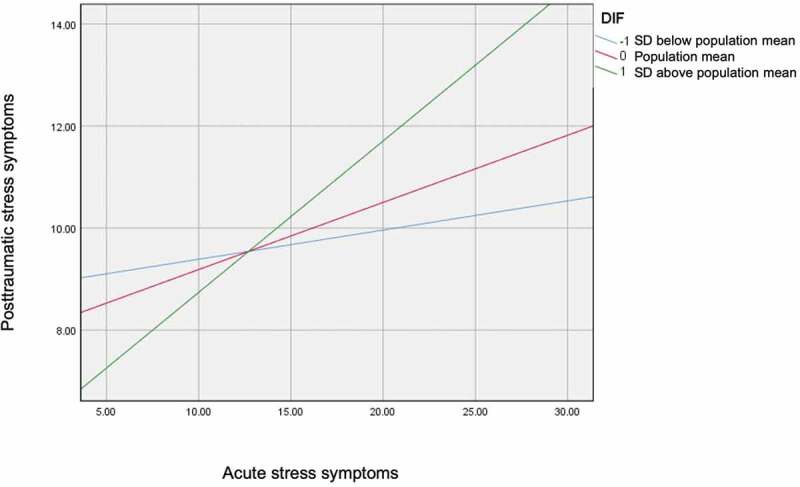
The linear regression model explained 23% of the variance in MI-induced PTSS-symptoms ((6.109) = 5.58, < 0.001, = 0.23. ASS was significantly related to PTSS severity ( (152) = < 0.001). The scores of the TAS-20 subscale difficulties identifying feelings (DIF) were found to significantly moderate this relationship ( = 0.03, = 0.04). The scores of TAS-20 subscales DDF and EOT as well as the TAS-20 total score had no influence on the relationship between ASS and PTSS (p > 0.05).
In MI patients with high levels of DIF, ASS predicted the development of PTSS. If replicated, the finding may inform emotion-oriented interventions to investigate whether increasing the capacity to identify feelings following acute MI could be beneficial in preventing the development of PTSS.
人们已经认识到,诸如急性心肌梗死(MI)等危及生命的医疗经历常常会导致急性应激障碍症状(ASS),进而可能引发创伤后应激症状(PTSS)的出现。先前的研究表明,各种创伤经历与述情障碍之间存在关联。述情障碍与心肌梗死患者的急性应激障碍症状和创伤后应激症状之间的关联尚不明确。
本研究旨在探讨述情障碍与有患创伤后应激障碍高风险的心肌梗死患者的心肌梗死诱发的急性应激障碍症状和创伤后应激症状之间的关联。
对154例患者进行了两次检查,一次在48小时内,另一次在急性心肌梗死后三个月。所有患者在心脏事件发生后48小时内完成了自评急性应激障碍量表(ASDS)。出院三个月后,所有患者完成了多伦多述情障碍量表(TAS - 20),并接受了临床医生管理的创伤后应激障碍量表(CAPS),这是一项用于评估创伤后应激症状严重程度的结构化访谈。进行了描述性统计、相关性分析、多元线性回归分析和调节分析。
线性回归模型解释了心肌梗死诱发的创伤后应激症状方差的23%(F(6,109)=5.58,p<0.001,R² = 0.23)。急性应激障碍症状与创伤后应激障碍严重程度显著相关(β(152)=...<0.001)。发现多伦多述情障碍量表的识别感受困难(DIF)子量表得分显著调节了这种关系(β = 0.03,p = 0.04)。多伦多述情障碍量表的难以描述情感和外向思维障碍子量表得分以及多伦多述情障碍量表总分对急性应激障碍症状与创伤后应激障碍症状之间的关系没有影响(p>0.05)。
在识别感受困难水平较高的心肌梗死患者中,急性应激障碍症状可预测创伤后应激障碍的发生。如果该研究结果得到重复验证,这一发现可能为以情感为导向的干预措施提供依据,以研究提高急性心肌梗死后识别感受的能力是否有助于预防创伤后应激障碍的发生。