Tafti Dawood, Kluckman Matthew, Dearborn Michael C, Hunninghake John, Clayton Sara
Radiology, Brooke Army Medical Center, Fort Sam Houston, USA.
Critical Care Medicine, Brooke Army Medical Center, Fort Sam Houston, USA.
Cureus. 2020 Dec 13;12(12):e12064. doi: 10.7759/cureus.12064.
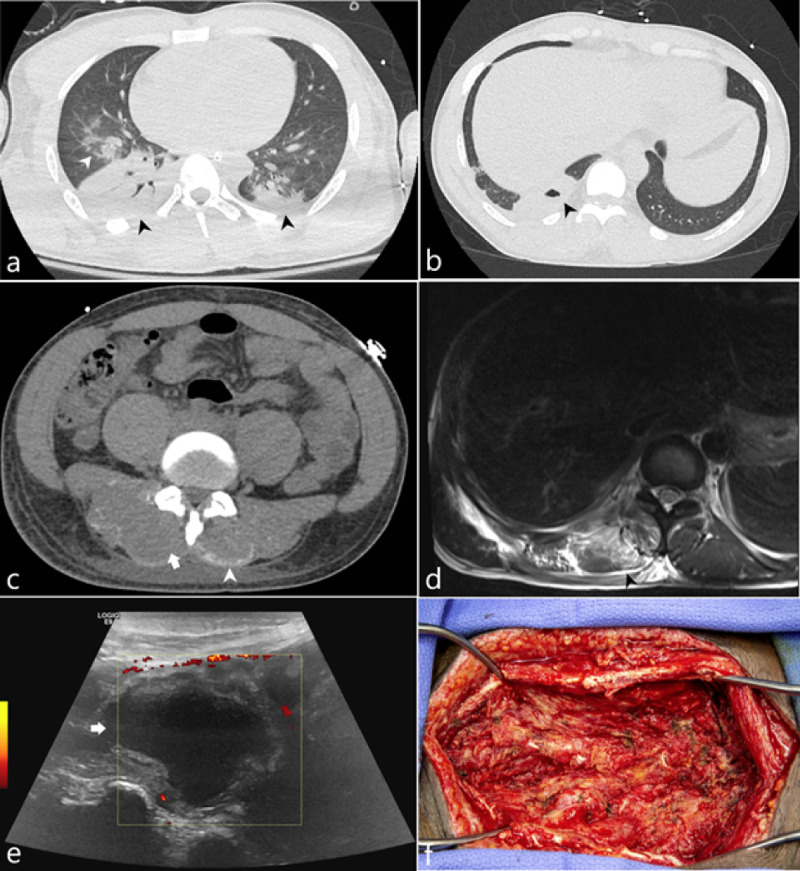
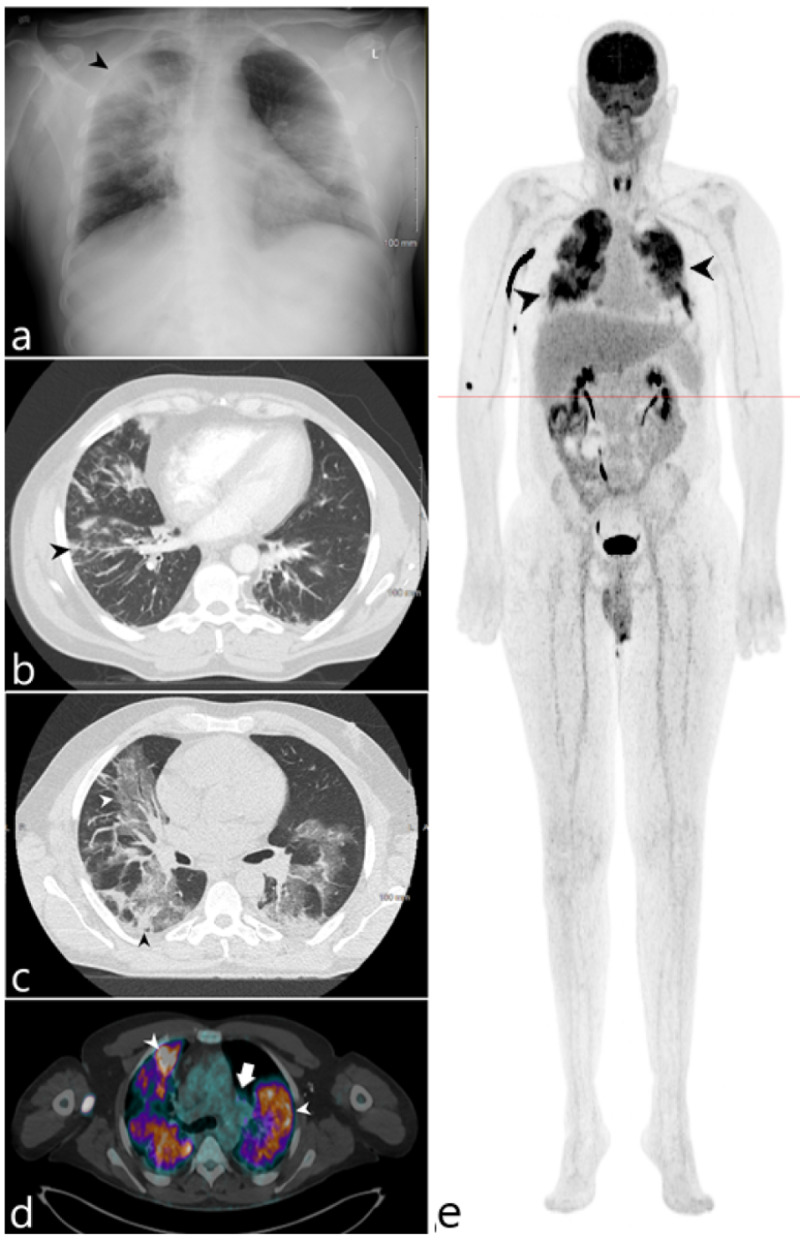
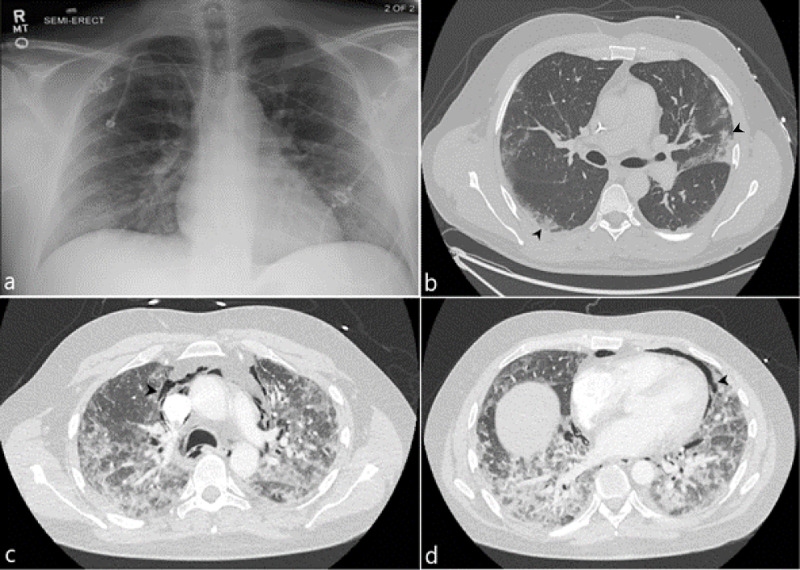
The novel COVID-19 infection has demonstrated a spectrum of complications involving vascular, inflammatory, infectious, and metabolic conditions. These complications range from mild loss of smell to more severe acute respiratory distress syndrome (ARDS). Patients with more severe complications often require sedation and mechanical ventilation. Growing research has revealed the role of active malignancy and disease-in-remission status as possible risk factors contributing to the morbidity and mortality in COVID-19 patients. In our descriptive case series, we present three unique cases of complicated COVID-19 infection in patients with hematologic-oncologic risk factors and review the imaging features of their complications. The first patient was a 33-year-old male with sickle cell trait who developed rhabdomyolysis and myonecrosis of the paraspinal muscle in the setting of a physical fitness test; he subsequently developed an abscess at this site, presumably exacerbated by the hypoxemic state of his COVID-19 pneumonia. Our second patient was a 37-year-old male with COVID-19 pneumonia and a history of stage IV Non-Hodgkin's lymphoma in remission who developed spontaneous pneumomediastinum in the absence of positive pressure ventilation. The third COVID-positive patient was a 54-year-old male with a past medical history significant for grade 1 follicular non-Hodgkin's lymphoma in remission with sputum culture positive for mycobacterium avium complex and bronchoscopy positive for candida growth. 18-FDG/PET imaging was performed and demonstrated diffuse intense uptake throughout the lungs reflecting both the COVID-19 pneumonia and the multimicrobial superinfection.
新型冠状病毒肺炎感染已表现出一系列并发症,涉及血管、炎症、感染和代谢状况。这些并发症从轻微的嗅觉丧失到更严重的急性呼吸窘迫综合征(ARDS)不等。并发症较严重的患者通常需要镇静和机械通气。越来越多的研究表明,活动性恶性肿瘤和疾病缓解状态可能是导致新冠肺炎患者发病和死亡的危险因素。在我们的描述性病例系列中,我们介绍了三例具有血液肿瘤危险因素的新冠肺炎复杂感染的独特病例,并回顾了其并发症的影像学特征。首例患者是一名33岁男性,具有镰状细胞性状,在体能测试时发生了椎旁肌横纹肌溶解和肌坏死;随后该部位出现脓肿,推测是由其新冠肺炎肺炎的低氧状态加剧所致。第二例患者是一名37岁男性,患有新冠肺炎肺炎,有IV期非霍奇金淋巴瘤缓解病史,在没有正压通气的情况下发生了自发性纵隔气肿。第三例新冠阳性患者是一名54岁男性,既往病史显示有1级滤泡性非霍奇金淋巴瘤缓解,痰培养鸟分枝杆菌复合群阳性,支气管镜检查念珠菌生长阳性。进行了18-FDG/PET成像,结果显示肺部弥漫性强烈摄取,反映了新冠肺炎肺炎和多重微生物重叠感染。