Friedman Ari B, Barfield Deidre, David Guy, Diller Thomas, Gunnarson Candace, Liu Miao, Vicidomina Benjamin V, Zhang Ruthann, Zhang Yuan, Nigam Somesh C
Perelman School of Medicine University of Pennsylvania Philadelphia Pennsylvania USA.
Leonard Davis Institute of Health Economics University of Pennsylvania Philadelphia Pennsylvania USA.
J Am Coll Emerg Physicians Open. 2021 Jan 14;2(1):e12349. doi: 10.1002/emp2.12349. eCollection 2021 Feb.
COVID-19 has been associated with excess mortality among patients not diagnosed with COVID-19, suggesting disruption of acute health care provision may play a role.
To determine the degree of declines in emergency department (ED) visits attributable to COVID-19 and determine whether these declines were concentrated among patients with fewer comorbidities and lower severity visits.
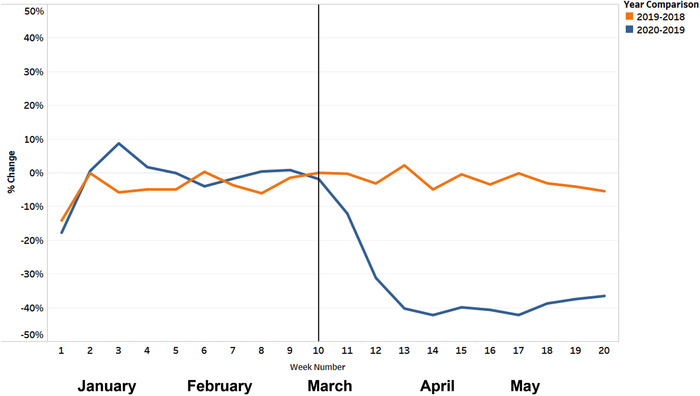
We conducted a differences-in-differences analysis of all commercial health insurance claims for ED visits in the first 20 weeks of 2018, 2019, and 2020. The intervention period began March 9 (week 11) of 2020, following state stay-at-home orders.
We analyzed claims from Blue Cross Blue Shield of Louisiana (BCBSLA), located in a state with an early US COVID-19 outbreak. Visit and patient risk was assessed through comorbidities previously described as increasing the risk of COVID-19 decompensation, the hospital location's COVID-19 outbreak status, and the Ambulatory Care Sensitive Condition algorithm.
The study population comprised all ED visits from all BCBSLA members, whether admitted or discharged. There were 332,917 ED visits over the study period. The study population spanned member demographics including sex, age, and geography. Uninsured adults were not included due to data limitations.
The COVID-19 outbreak beginning March 9, 2020 in Louisiana.
The main outcome of interest for this analysis is the difference (percent change) in all ED visits, categorized as either respiratory or non-respiratory, from week 1-20 in 2019 and week 1-10 in 2020, compared to week 11-20 in 2020.
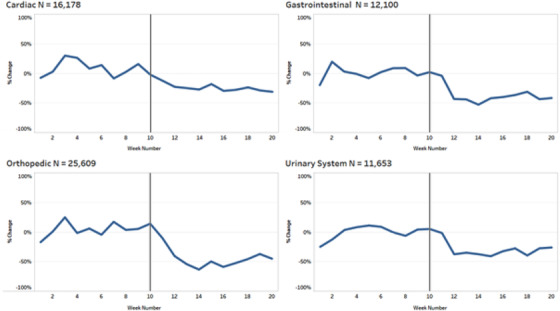
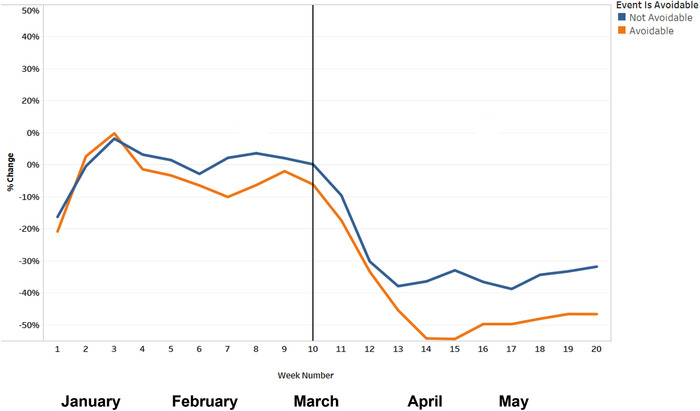
In this differences-in-differences study using data from a commercial health insurer, we found that non-respiratory ED visits declined by 39%, whereas respiratory visits did not experience a significant decline. Visits that were potentially deferrable or from lower risk patient populations showed greater declines, but even high-risk patients and non-avoidable visits experienced large declines in non-respiratory ED visits. Non-respiratory ED visits declined by only 18% in areas experiencing COVID outbreak.
COVID-19 has resulted in significant avoidance of ED care, comprising a mix of deferrable and high severity care. Hospital and public health pronouncements should emphasize appropriate care seeking.
新冠病毒病(COVID-19)与未被诊断为COVID-19的患者的超额死亡率相关,这表明急性医疗服务的中断可能起到了一定作用。
确定因COVID-19导致的急诊科(ED)就诊量下降程度,并确定这些下降是否集中在合并症较少和病情较轻的患者中。
我们对2018年、2019年和2020年第1至20周所有商业医疗保险的ED就诊索赔进行了双重差分分析。干预期从2020年3月9日(第11周)开始,即各州发布居家令之后。
我们分析了位于美国早期出现COVID-19疫情的路易斯安那州蓝十字蓝盾公司(BCBSLA)的索赔数据。通过先前描述的增加COVID-19失代偿风险的合并症、医院所在地区的COVID-19疫情状况以及门诊护理敏感状况算法来评估就诊情况和患者风险。
研究人群包括BCBSLA所有成员的所有ED就诊,无论其入院还是出院。研究期间共有332,917次ED就诊。研究人群涵盖了成员的人口统计学特征,包括性别、年龄和地理位置。由于数据限制,未纳入未参保成年人。
2020年3月9日在路易斯安那州开始的COVID-19疫情。
本分析关注的主要结局是2019年第1至20周和2020年第1至10周所有ED就诊(分为呼吸类或非呼吸类)与2020年第11至20周相比的差异(百分比变化)。
在这项使用商业健康保险公司数据的双重差分研究中,我们发现非呼吸类ED就诊量下降了39%,而呼吸类就诊量没有显著下降。可能可推迟的就诊或来自低风险患者群体的就诊下降幅度更大,但即使是高风险患者和不可避免的就诊,非呼吸类ED就诊量也大幅下降。在出现COVID疫情的地区,非呼吸类ED就诊量仅下降了18%。
COVID-19导致大量患者避免前往ED就诊,包括可推迟和高严重程度的护理。医院和公共卫生部门的声明应强调寻求适当的医疗护理。