Centre for Innovation and Leadership, Faculty of Health Sciences, University of Southampton, Building 45, Room 2035, Highfield Campus, S017 1BJ, Southampton, UK.
Critical Care Anaesthesia and Perioperative Research Unit and Integrative Physiology, Clinical Experimental Sciences and NIHR Respiratory Biomedical Research Unit, University Hospital Southampton NHS Foundation Trust and University Hospital Southampton, Southampton, UK.
BMC Anesthesiol. 2021 Jan 25;21(1):27. doi: 10.1186/s12871-020-01227-z.
Early rehabilitation can reduce ventilation duration and improve functional outcomes in critically ill patients. Upper limb strength is associated with ventilator weaning. Passive muscle loading may preserve muscle fibre function, help recover peripheral muscle strength and improve longer term, post-hospital discharge function capacity. The physiological effects of initiating rehabilitation soon after physiological stabilisation of these patients can be concerning for clinicians. This study investigated the feasibility of measuring metabolic demand and the safety and feasibility of early upper limb passive ergometry. An additional comparison of results, achieved from simultaneous application of the methods, is reported.
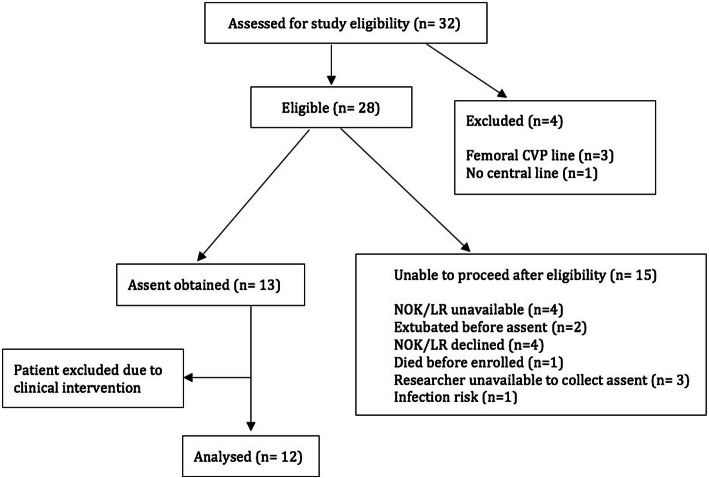
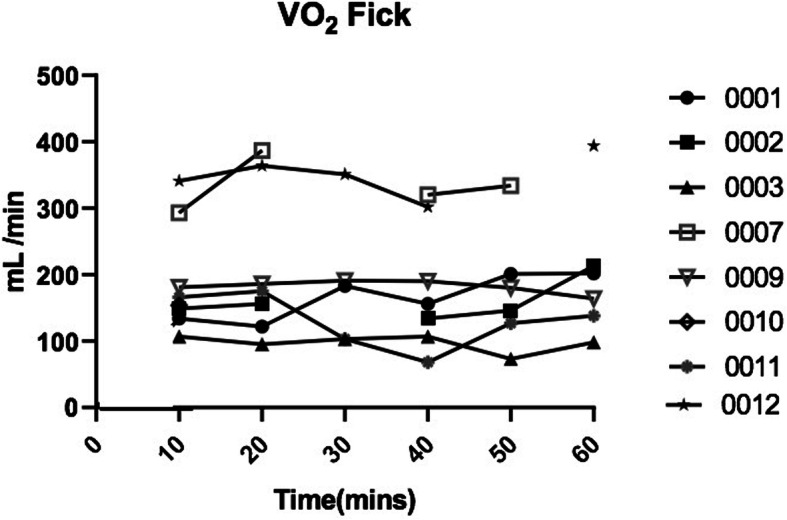
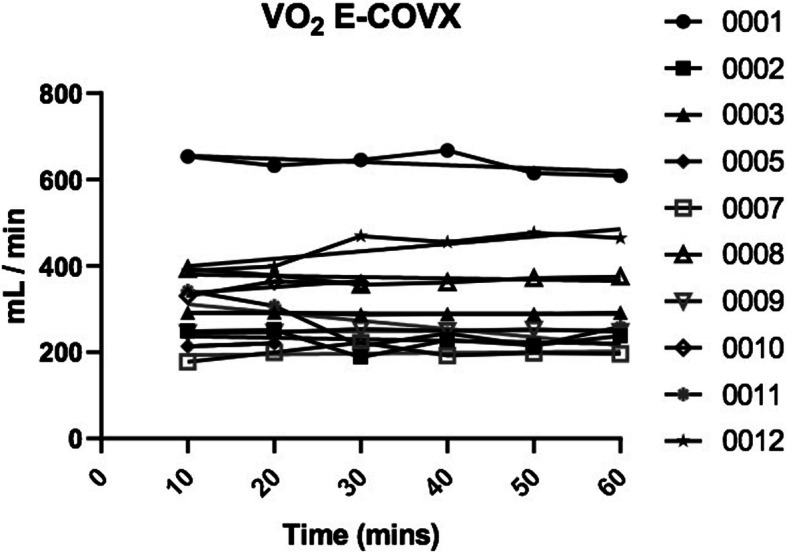
This was an observational feasibility study undertaken in an acute teaching hospital's General Intensive Care Unit in the United Kingdom. Twelve haemodynamically stable, mechanically ventilated patients underwent 30 minutes of arm ergometry. Cardiovascular and respiratory parameters were monitored. A Friedman test identified changes in physiological parameters. A metabolic cart was attached to the ventilator to measure oxygen uptake. Oxygen uptake was concurrently calculated by the reverse Fick method, utilising cardiac output from the LiDCO™ and paired mixed venous and arterial samples. A comparison of the two methods was made. Data collection began 10 minutes before ergometry and continued to recovery. Paired mixed venous and arterial samples were taken every 10 minutes.
Twelve patients were studied; 9 male, median age 55 years, range (27-82), median APACHE score 18.5, range (7-31), median fraction inspired oxygen 42.5%, range (28-60). Eight patients were receiving noradrenaline. Mean dose was 0.07 mcg/kg/min, range (0.01-0.15). Early ergometry was well tolerated. There were no clinically significant changes in respiratory, haemodynamic or metabolic variables pre ergometry to end recovery. There was no significant difference between the two methods of calculating VO (p = 0.70).
We report the feasibility of using the reverse Fick method and indirect calorimetry to measure metabolic demand during early physical rehabilitation of critically ill patients. More research is needed to ascertain the most reliable method. Minimal change in metabolic demand supports the safety and feasibility of upper limb ergometry. These results will inform future study designs for further research into exercise response in critically ill patients.
Clinicaltrials.gov No. NCT04383171. Registered on 06 May 2020 - Retrospectively registered. http://www.clinicaltrials.gov .
早期康复可以减少危重症患者的通气时间并改善其功能结局。上肢力量与呼吸机脱机相关。被动肌肉负荷可能有助于保持肌肉纤维功能,帮助恢复外周肌肉力量,并改善更长时间的出院后功能能力。对于临床医生来说,这些患者在生理稳定后立即开始康复治疗的生理影响可能令人担忧。本研究旨在调查测量代谢需求的可行性,以及早期上肢被动运动的安全性和可行性。同时报告了同时应用这些方法获得的结果的额外比较。
这是一项在英国一家急性教学医院综合重症监护病房进行的观察性可行性研究。12 名血流动力学稳定、机械通气的患者接受了 30 分钟的手臂运动。监测心血管和呼吸参数。弗里德曼检验确定了生理参数的变化。将代谢箱连接到呼吸机上以测量耗氧量。同时利用 LiDCO™ 测量心输出量和配对混合静脉及动脉样本,通过逆向 Fick 法计算耗氧量。比较了这两种方法。数据采集在运动前 10 分钟开始,并持续到恢复。每 10 分钟采集一次配对的混合静脉和动脉样本。
研究共纳入 12 名患者,其中 9 名男性,中位年龄 55 岁(范围 27-82),中位急性生理学和慢性健康状况评分系统(APACHE) 18.5 分(范围 7-31),中位吸入氧分数 42.5%(范围 28-60)。8 名患者正在接受去甲肾上腺素。平均剂量为 0.07 mcg/kg/min(范围 0.01-0.15)。早期运动耐受良好。在运动前至恢复结束期间,呼吸、血流动力学或代谢变量没有出现临床上有意义的变化。两种计算 VO2 的方法之间没有显著差异(p=0.70)。
我们报告了在危重症患者早期身体康复期间使用逆向 Fick 法和间接测热法测量代谢需求的可行性。需要进一步研究以确定最可靠的方法。代谢需求的微小变化支持上肢运动的安全性和可行性。这些结果将为进一步研究危重症患者的运动反应提供信息。
Clinicaltrials.gov 编号 NCT04383171。2020 年 5 月 6 日注册-回顾性注册。http://www.clinicaltrials.gov。