Collings Nikki, Cusack Rebecca
Department of Physiotherapy, University Hospital Southampton NHS Foundation Trust, Tremona Road, SO16 6YD Southampton, UK ; Anaesthesia and Critical Care Research Unit, University Hospital Southampton NHS Foundation Trust, Tremona Road, SO16 6YD Southampton, UK ; Integrative Physiology and Critical Illness Group, Clinical and Experimental Sciences, University of Southampton, University Hospital Southampton, Tremona Road, SO16 6YD Southampton, UK.
Anaesthesia and Critical Care Research Unit, University Hospital Southampton NHS Foundation Trust, Tremona Road, SO16 6YD Southampton, UK ; Integrative Physiology and Critical Illness Group, Clinical and Experimental Sciences, University of Southampton, University Hospital Southampton, Tremona Road, SO16 6YD Southampton, UK ; Southampton NIHR Respiratory Biomedical Research Unit, University Hospital Southampton, Tremona Road, SO16 6YD Southampton, UK.
BMC Anesthesiol. 2015 Jan 13;15(1):1. doi: 10.1186/1471-2253-15-1. eCollection 2015.
Early mobilisation of critically ill patients is safe and beneficial, but the metabolic cost of exercise remains unquantified. This study compared the acute exercise response in critically ill participants during passive and active sitting.
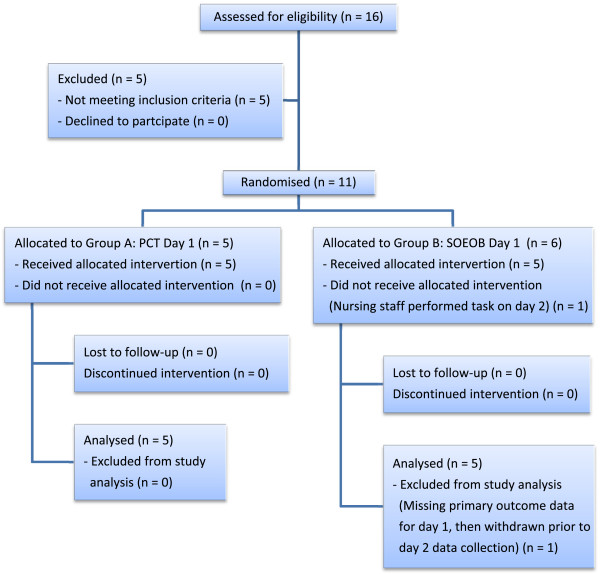
We conducted a prospective, randomised, cross-over study, in ventilated patients receiving rehabilitative physiotherapy. Ten participants completed a passive chair transfer, or a sit on the edge of the bed, followed by the alternate exercise activity on the consecutive day. The primary outcome measure was oxygen consumption.
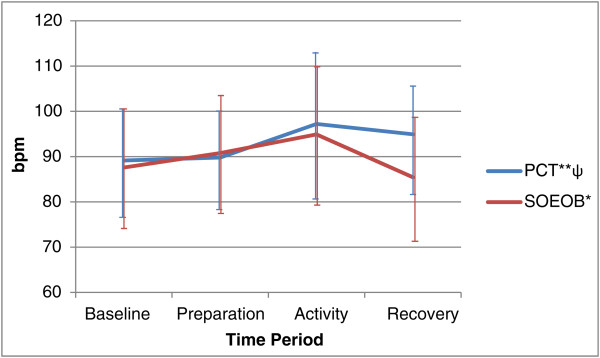
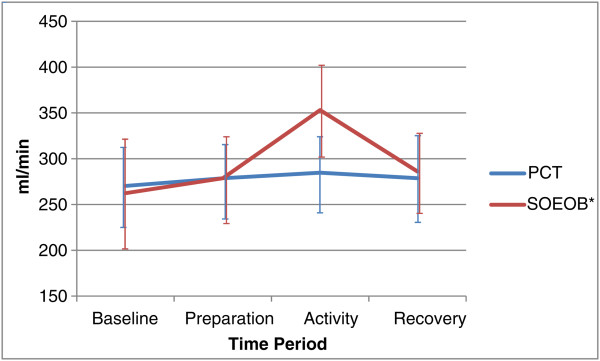
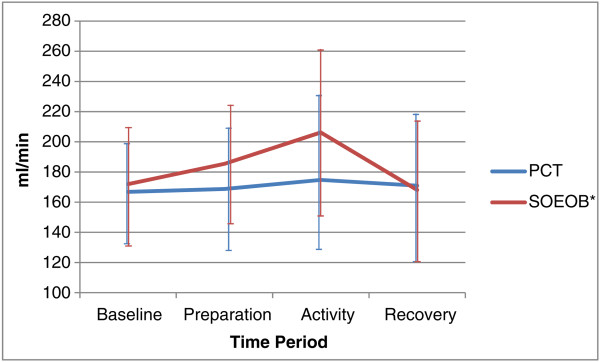
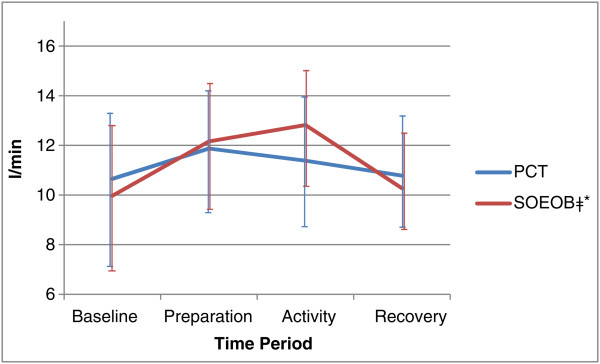
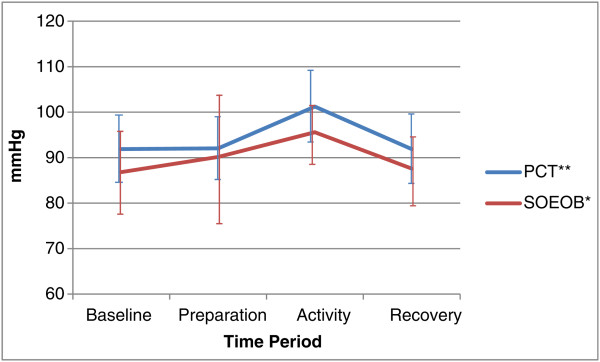
In comparison to resting supine, a passive chair transfer elicited no change in oxygen consumption, carbon dioxide production or minute ventilation; but mean arterial pressure (91.86 mmHg (95% CI 84.61 to 99.10) to 101.23 mmHg (95% CI 93.35 to 109.11) (p = 0.002)) and heart rate (89.13 bpm (95% CI 77.14 to 101.13) to 97.21 bpm (95% CI 81.22 to 113.20) (p = 0.008)) increased. Sitting on the edge of the bed resulted in significant increases in oxygen consumption (262.33 ml/min (95% CI 201.97 to 322.70) to 353.02 ml/min (95% CI 303.50 to 402.55), p = 0.002), carbon dioxide production (171.93 ml/min (95% CI 131.87 to 211.98) to 206.23 ml/min (95% CI 151.03 to 261.43), p = 0.026), minute ventilation (9.97 l/min (95% CI 7.30 to 12.65) to 12.82 l/min (95% CI 10.29 to 15.36), p < 0.001), mean arterial pressure (86.81 mmHg (95% CI 77.48 to 96.14) to 95.59 mmHg (95% CI 88.62 to 102.56), p = 0.034) and heart rate (87.60 bpm (95% CI 73.64 to 101.56) to 94.91 bpm (95% CI 79.57 to 110.25), p = 0.007). When comparing the 2 activities, sitting on the edge of the bed elicited a significantly larger increase in oxygen consumption (90.69 ml/min (95% CI 44.04 to 137.34) vs 14.43 ml/min (95% CI -27.28 to 56.14), p = 0.007) and minute ventilation (2.85 l/min (95% CI 1.70 to 3.99) vs 0.74 l/min (95% CI -0.92 to 1.56), p = 0.012).
Sitting on the edge of the bed is a more metabolically demanding activity than a passive chair transfer in critically ill patients.
危重症患者早期活动是安全且有益的,但运动的代谢成本仍未得到量化。本研究比较了危重症参与者在被动坐和主动坐期间的急性运动反应。
我们对接受康复物理治疗的通气患者进行了一项前瞻性、随机、交叉研究。10名参与者完成了一次被动椅转移或床边坐,然后在连续的第二天进行交替的运动活动。主要结局指标是耗氧量。
与静息仰卧位相比,被动椅转移时耗氧量、二氧化碳产生量或分钟通气量均无变化;但平均动脉压(从91.86 mmHg(95%CI 84.61至99.10)升至101.23 mmHg(95%CI 93.35至109.11)(p = 0.002))和心率(从89.13次/分钟(95%CI 77.14至101.13)升至97.21次/分钟(95%CI 81.22至113.20)(p = 0.008))增加。床边坐导致耗氧量(从262.33 ml/分钟(95%CI 201.97至322.70)增至353.02 ml/分钟(95%CI 303.50至402.55),p = 0.002)、二氧化碳产生量(从171.93 ml/分钟(95%CI 131.87至211.98)增至206.23 ml/分钟(95%CI 151.03至261.43),p = 0.026)、分钟通气量(从9.97 l/分钟(95%CI 7.30至12.65)增至12.82 l/分钟(95%CI 10.29至15.36),p < 0.oo1)、平均动脉压(从86.81 mmHg(95%CI 77.48至96.14)升至95.59 mmHg(95%CI 88.62至102.56),p = 0.034)和心率(从87.60次/分钟(95%CI 73.64至101.56)升至94.91次/分钟(95%CI 79.57至110.25),p = 0.007)显著增加。比较这两种活动时,床边坐引起的耗氧量(90.69 ml/分钟(95%CI 44.04至137.34)对14.43 ml/分钟(95%CI -27.28至56.14),p = 0.007)和分钟通气量(2.85 l/分钟(95%CI 1.70至3.99)对0.74 l/分钟(95%CI -0.92至1.56),p = 0.012)增加显著更大。
对于危重症患者,床边坐比被动椅转移的代谢需求更高。