Department of Intensive Care Medicine, Radboud University Medical Center, 6500HB, Nijmegen, The Netherlands.
Radboud Center for Infectious Diseases, Radboud University Medical Center, 6500HB, Nijmegen, The Netherlands.
Int J Obes (Lond). 2021 Mar;45(3):687-694. doi: 10.1038/s41366-021-00747-z. Epub 2021 Jan 25.
BACKGROUND/OBJECTIVES: Obesity appears to be an independent risk factor for ICU admission and a severe disease course in COVID-19 patients. An aberrant inflammatory response and impaired respiratory function have been suggested as underlying mechanisms. We investigated whether obesity is associated with differences in inflammatory, respiratory, and clinical outcome parameters in critically ill COVID-19 patients.
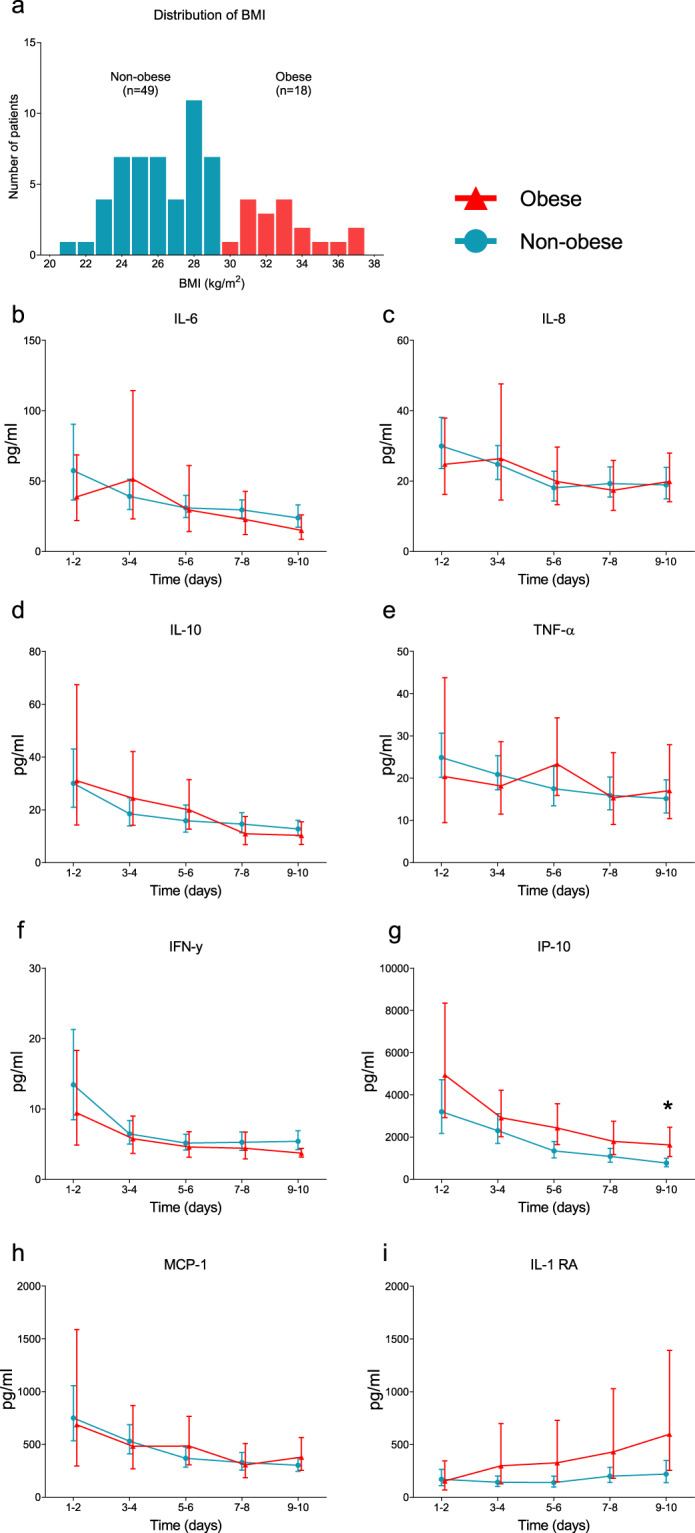
SUBJECTS/METHODS: Sixty-seven COVID-19 ICU patients were divided into obese (BMI ≥ 30 kg/m, n = 18, 72% class I obesity, 28% class II obesity) and non-obese (BMI < 30 kg/m, n = 49) groups. Concentrations of circulating interleukin (IL)-6, IL-8, IL-10, tumor necrosis factor alpha (TNF-α), interferon gamma (IFN-γ), interferon gamma-induced protein (IP)-10, monocyte chemoattractant protein (MCP)-1, and IL-1 receptor antagonist (RA) were determined from ICU admission until 10 days afterward, and routine laboratory and clinical parameters were collected.
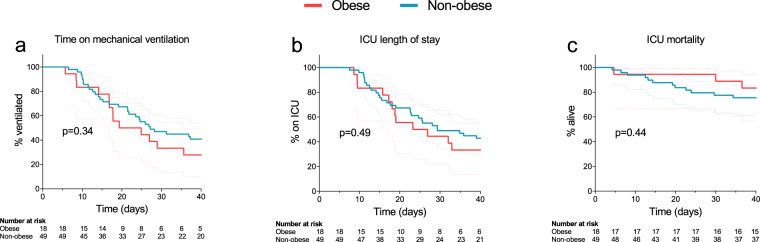
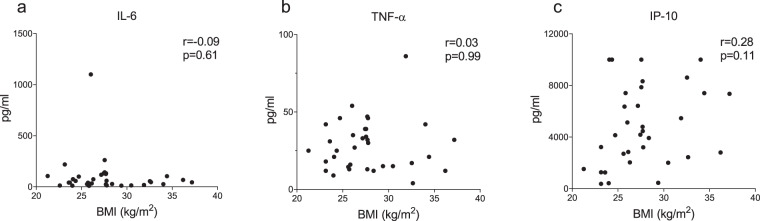
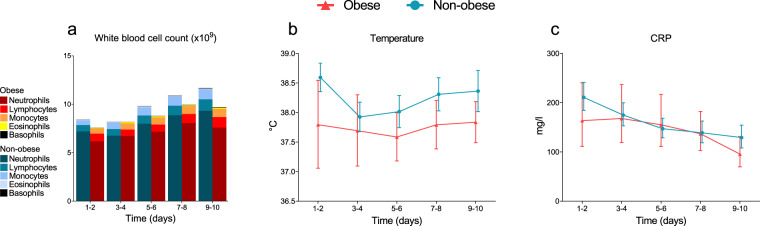
BMI was 32.6 [31.2-34.5] and 26.0 [24.4-27.7] kg/m in the obese and non-obese group, respectively. Apart from temperature, which was significantly lower in obese patients (38.1 [36.9-38.9] vs. 38.7 [38.0 -39.5] °C, p = 0.02), there were no between-group differences on ICU admission. Plasma cytokine concentrations declined over time (p < 0.05 for all), but no differences between obese and non-obese patients were observed. Also, BMI did not correlate with the cytokine response (IL-6 r = 0.09, p = 0.61, TNF-α r = 0.03, p = 0.99, IP-10 r = 0.28, p = 0.11). The kinetics of clinical inflammatory parameters and respiratory mechanics were also similar in both groups. Finally, no differences in time on ventilator, ICU length of stay or 40-day mortality between obese and non-obese patients were apparent.
In COVID-19 patients requiring mechanical ventilation in the ICU, a higher BMI is not related to a different immunological response, unfavorable respiratory mechanics, or impaired outcome.
背景/目的:肥胖似乎是 COVID-19 患者入住 ICU 和病情严重的独立危险因素。异常的炎症反应和呼吸功能受损被认为是潜在的机制。我们研究了肥胖是否与危重症 COVID-19 患者的炎症、呼吸和临床结局参数存在差异有关。
对象/方法:67 例 COVID-19 ICU 患者分为肥胖组(BMI≥30kg/m2,n=18,72%为 I 度肥胖,28%为 II 度肥胖)和非肥胖组(BMI<30kg/m2,n=49)。从 ICU 入院开始至入院后 10 天,测定循环白细胞介素(IL)-6、IL-8、IL-10、肿瘤坏死因子-α(TNF-α)、干扰素γ(IFN-γ)、干扰素γ诱导蛋白(IP)-10、单核细胞趋化蛋白-1(MCP-1)和白细胞介素-1 受体拮抗剂(IL-1RA)的浓度,并收集常规实验室和临床参数。
肥胖组和非肥胖组的 BMI 分别为 32.6[31.2-34.5]kg/m2和 26.0[24.4-27.7]kg/m2。肥胖患者的体温明显较低(38.1[36.9-38.9]℃与 38.7[38.0-39.5]℃,p=0.02),除此之外,两组患者在 ICU 入院时无差异。血浆细胞因子浓度随时间下降(所有 p<0.05),但肥胖组和非肥胖组之间无差异。此外,BMI 与细胞因子反应无相关性(IL-6 r=0.09,p=0.61,TNF-α r=0.03,p=0.99,IP-10 r=0.28,p=0.11)。两组患者临床炎症参数和呼吸力学的动力学也相似。最后,肥胖组和非肥胖组患者的呼吸机使用时间、ICU 住院时间或 40 天死亡率无差异。
在需要 ICU 机械通气的 COVID-19 患者中,较高的 BMI 与不同的免疫反应、不利的呼吸力学或较差的预后无关。