Department of General Practice, Monash University, Notting Hill, Victoria, Australia.
National Centre for Antimicrobial Stewardship (NCAS), The Peter Doherty Institute for Infection and Immunity, Melbourne, Victoria, Australia.
Prim Health Care Res Dev. 2021 Jan 28;22:e2. doi: 10.1017/S1463423620000687.
Rising antimicrobial resistance (AMR) in primary care is a growing concern and a threat to community health. The rise of AMR can be slowed down if general practitioners (GPs) and community pharmacists (CPs) could work as a team to implement antimicrobial stewardship (AMS) programs for optimal use of antimicrobial(s). However, the evidence supporting a GP pharmacist collaborative AMS implementation model (GPPAS) in primary care remains limited.
With an aim to design a GPPAS model in Australia, this paper outlines how this model will be developed.
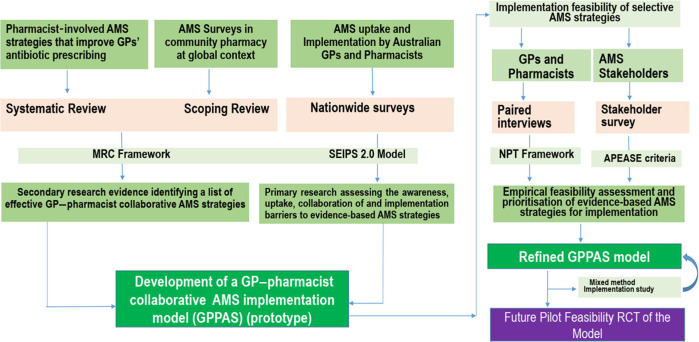
This exploratory study undertakes a systematic review, a scoping review, nationwide surveys, and qualitative interviews to design the model. Medical Research Council (MRC) framework and Normalization Process Theory are utilized as guides. Reviews will identify the list of effective GPPAS interventions. Two AMS surveys and paired interviews of GPs and CPs across Australia will explore their convergent and divergent views about the GPPAS interventions, attitudes towards collaboration in AMS and the perceived challenges of implementing GPPAS interventions. Systems Engineering Initiative for Patient Safety (SEIPS 2.0) model and factor analyses will guide the structure of GPPAS model through identifying the determinants of GPPAS uptake. The implementable GPPAS strategies will be selected based on empirical feasibility assessment by AMS stakeholders using the APEASE (Affordability, Practicability, Effectiveness and cost-effectiveness, Acceptability, Side-effects and safety, Equity) criteria.
The GPPAS model might have potential implications to inform how to better involve GPs and CPs in AMS, and, to improve collaborative services to optimize antimicrobial use and reduce AMR in primary care.
初级保健中抗菌药物耐药性(AMR)的上升是一个日益令人担忧的问题,也是社区健康的威胁。如果全科医生(GP)和社区药剂师(CP)能够合作实施抗菌药物管理(AMS)计划,以优化抗菌药物的使用,那么 AMR 的上升速度可以减缓。然而,支持初级保健中 GP 药剂师合作抗菌药物管理实施模式(GPPAS)的证据仍然有限。
旨在设计澳大利亚的 GPPAS 模型,本文概述了如何开发该模型。
这项探索性研究通过系统评价、范围综述、全国性调查和定性访谈来设计模型。医学研究委员会(MRC)框架和规范化进程理论被用作指导。综述将确定有效的 GPPAS 干预措施清单。在澳大利亚进行两次 AMS 调查和 GP 和 CP 的配对访谈,以探讨他们对 GPPAS 干预措施的趋同和分歧观点、对 AMS 合作的态度以及实施 GPPAS 干预措施的感知挑战。通过确定 GPPAS 采用的决定因素,系统工程患者安全倡议(SEIPS 2.0)模型和因子分析将指导 GPPAS 模型的结构。基于 AMS 利益相关者使用 APEASE(可负担性、可行性、有效性和成本效益、可接受性、副作用和安全性、公平性)标准对可实施的 GPPAS 策略进行实证可行性评估,选择可实施的 GPPAS 策略。
GPPAS 模型可能具有潜在的意义,可以告知如何更好地让 GP 和 CP 参与 AMS,并改善协作服务,以优化初级保健中的抗菌药物使用并降低 AMR。