Department of Hepatobiliary Pancreatic and Transplant Surgery, Mie University Graduate School of Medicine, Tsu, Mie, Japan.
PLoS One. 2021 Jan 28;16(1):e0245946. doi: 10.1371/journal.pone.0245946. eCollection 2021.
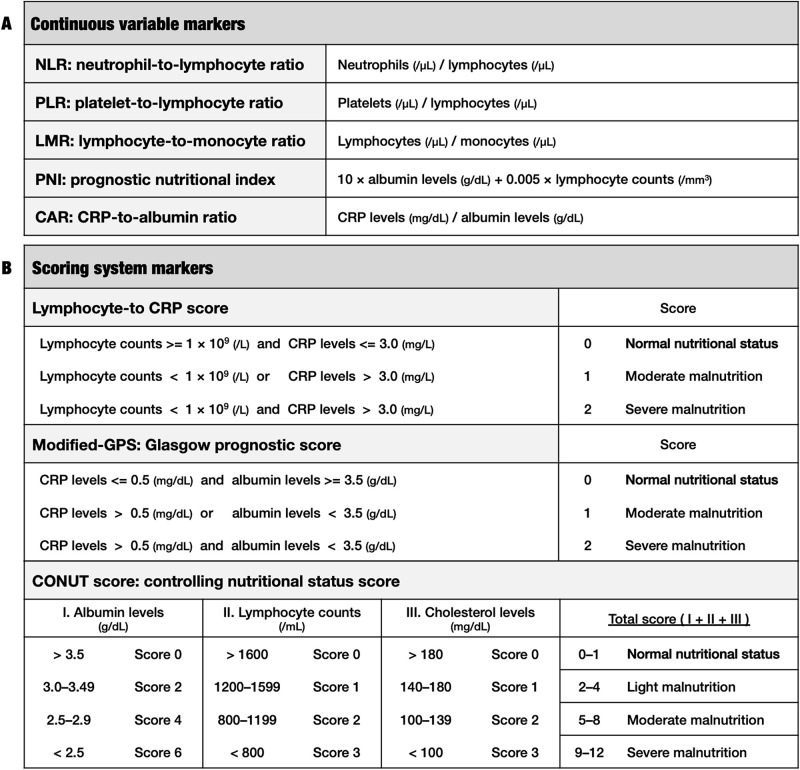
In many malignancies including intrahepatic cholangiocarcinoma (iCCA), prognostic significance of host-related inflammatory / immunonutritional markers have attracted a lot of attention. However, it is unclear which is the strongest prognostic indicator for iCCA among these markers. The aim of this study was to firstly evaluate the prognostic utility of inflammatory / immunonutritional markers in resected iCCA patients using a multiple comparison in addition to a new marker, lymphocyte-to-C-reactive protein (CRP) score.
A total of sixty iCCA patients, who underwent surgical resection between October 2004 and April 2019, were enrolled in this study. Their clinical and pathological data were retrospectively assessed using univariate and multivariate analysis to determine prognostic predictors for disease specific survival (DSS). Moreover, these patients, who were divided into high and low groups based on lymphocyte-to-CRP score, were compared these survival outcomes using Kaplan-Meier analysis with a log-rank test.
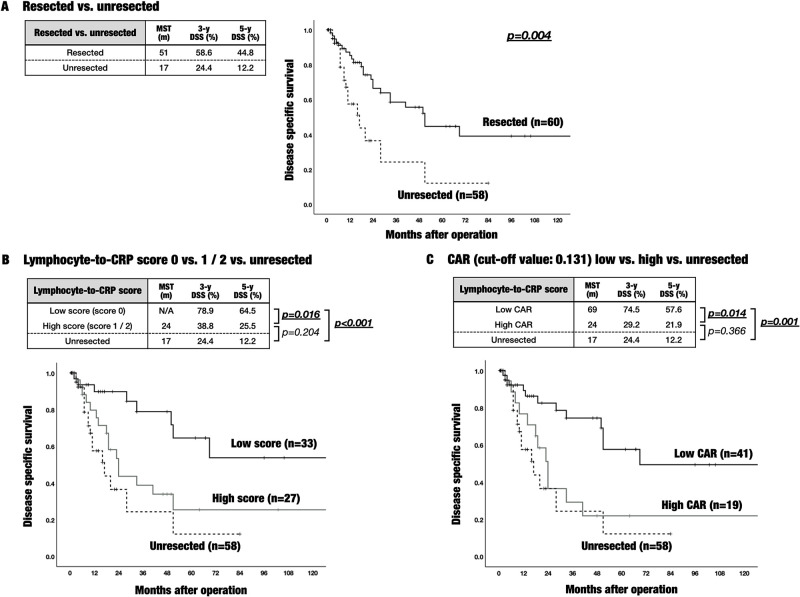
In multivariate analysis, the significant prognostic factors were preoperative lymphocyte-to-CRP score (p = 0.008), preoperative CRP-to-albumin ratio (CAR; p = 0.017), pathological T category (p = 0.003), and pathological vascular invasion (p < 0.001). Resected iCCA patients with a low lymphocyte-to-CRP score (score 0) had significant better prognosis than patients with a high score (score 1 or 2) (p = 0.016). Notably, the mortality of the high lymphocyte-to-CRP score group did not show statistically difference from the poor mortality of unresected iCCA patients (p = 0.204).
Preoperative lymphocyte-to-CRP score was the strongest prognostic indicator in iCCA patients with surgical resection. In these patients, early intervention with nutritional support should be considered prior to operation.
在包括肝内胆管细胞癌(iCCA)在内的许多恶性肿瘤中,宿主相关炎症/免疫营养标志物的预后意义引起了广泛关注。然而,这些标志物中哪一个是 iCCA 最强的预后指标尚不清楚。本研究的目的是首先使用多种比较方法评估炎症/免疫营养标志物在接受手术切除的 iCCA 患者中的预后作用,其中包括一个新标志物——淋巴细胞与 C 反应蛋白(CRP)比值评分。
本研究共纳入 60 例于 2004 年 10 月至 2019 年 4 月期间接受手术切除的 iCCA 患者。回顾性分析其临床病理资料,采用单因素和多因素分析确定疾病特异性生存(DSS)的预后预测因素。此外,根据淋巴细胞与 CRP 比值评分将这些患者分为高低两组,通过 Kaplan-Meier 分析和对数秩检验比较这些生存结果。
多因素分析结果显示,术前淋巴细胞与 CRP 比值(p = 0.008)、术前 CRP 与白蛋白比值(CAR;p = 0.017)、病理 T 分期(p = 0.003)和病理血管侵犯(p < 0.001)是显著的预后因素。淋巴细胞与 CRP 比值低(评分 0)的 iCCA 患者与比值高(评分 1 或 2)的患者相比,预后显著更好(p = 0.016)。值得注意的是,高淋巴细胞与 CRP 比值组的死亡率与未接受手术切除的 iCCA 患者的高死亡率之间无统计学差异(p = 0.204)。
术前淋巴细胞与 CRP 比值是接受手术切除的 iCCA 患者最强的预后指标。对于这些患者,在手术前应考虑进行营养支持的早期干预。