Kozlowska Kasia, Chudleigh Catherine, McClure Georgia, Maguire Ann M, Ambler Geoffrey R
Department of Psychological Medicine, The Children's Hospital at Westmead, Westmead, NSW, Australia.
Discipline of Child and Adolescent Health, University of Sydney Medical School, Darlington, NSW, Australia.
Front Psychol. 2021 Jan 12;11:582688. doi: 10.3389/fpsyg.2020.582688. eCollection 2020.
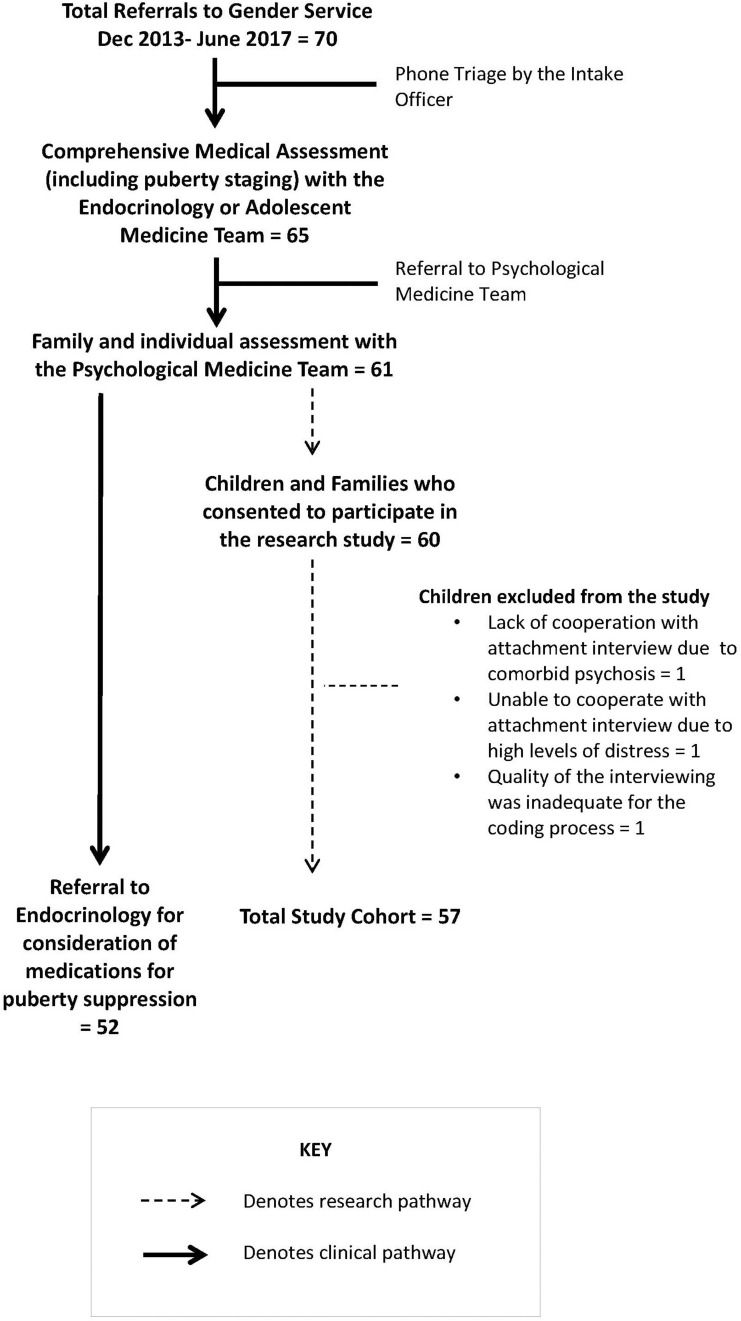
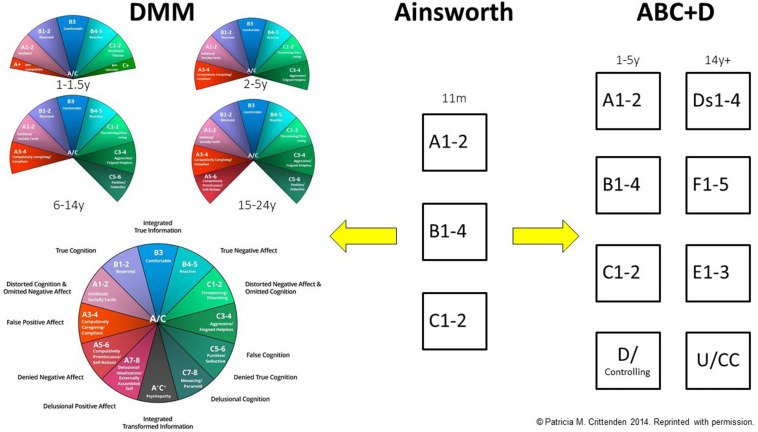
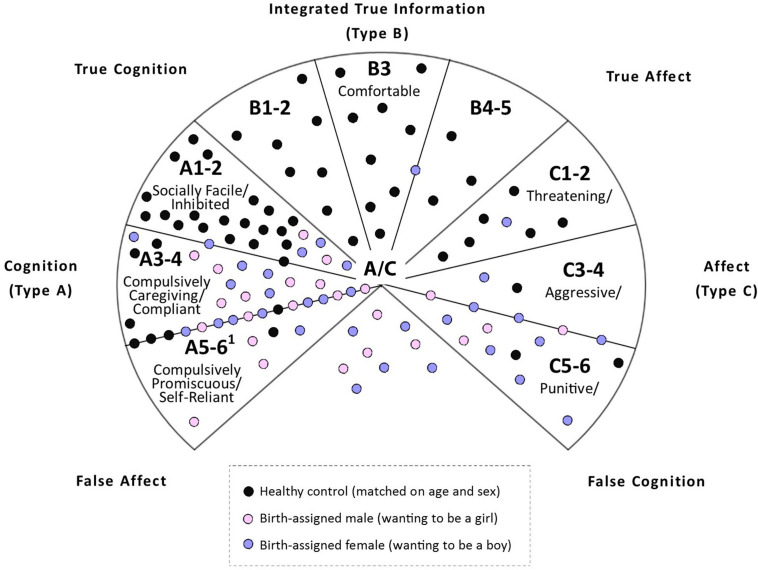
The current study examines patterns of attachment/self-protective strategies and rates of unresolved loss/trauma in children and adolescents presenting to a multidisciplinary gender service. Fifty-seven children and adolescents (8.42-15.92 years; 24 birth-assigned males and 33 birth-assigned females) presenting with gender dysphoria participated in structured attachment interviews coded using dynamic-maturational model (DMM) discourse analysis. The children with gender dysphoria were compared to age- and sex-matched children from the community (non-clinical group) and a group of school-age children with mixed psychiatric disorders (mixed psychiatric group). Information about adverse childhood experiences (ACEs), mental health diagnoses, and global level of functioning was also collected. In contrast to children in the non-clinical group, who were classified primarily into the normative attachment patterns (A1-2, B1-5, and C1-2) and who had low rates of unresolved loss/trauma, children with gender dysphoria were mostly classified into the high-risk attachment patterns (A3-4, A5-6, C3-4, C5-6, and A/C) (χ = 52.66; < 0.001) and had a high rate of unresolved loss/trauma (χ = 18.64; < 0.001). Comorbid psychiatric diagnoses ( = 50; 87.7%) and a history of self-harm, suicidal ideation, or symptoms of distress were also common. Global level of functioning was impaired (range 25-95/100; mean = 54.88; = 15.40; median = 55.00). There were no differences between children with gender dysphoria and children with mixed psychiatric disorders on attachment patterns (χ = 2.43; = 0.30) and rates of unresolved loss and trauma (χ = 0.70; = 0.40). analyses showed that lower SES, family constellation (a non-traditional family unit), ACEs-including maltreatment (physical abuse, sexual abuse, emotional abuse, neglect, and exposure to domestic violence)-increased the likelihood of the child being classified into a high risk attachment pattern. Akin to children with other forms of psychological distress, children with gender dysphoria present in the context of multiple interacting risk factors that include at-risk attachment, unresolved loss/trauma, family conflict and loss of family cohesion, and exposure to multiple ACEs.
本研究调查了前往多学科性别服务机构就诊的儿童和青少年的依恋模式/自我保护策略以及未解决的丧失/创伤发生率。57名患有性别焦虑症的儿童和青少年(年龄在8.42至15.92岁之间;出生时被指定为男性的有24人,出生时被指定为女性的有33人)参与了使用动态成熟模型(DMM)话语分析进行编码的结构化依恋访谈。将患有性别焦虑症的儿童与来自社区的年龄和性别匹配的儿童(非临床组)以及一组患有混合精神疾病的学龄儿童(混合精神疾病组)进行比较。还收集了有关童年不良经历(ACEs)、心理健康诊断和整体功能水平的信息。与主要被归类为规范依恋模式(A1-2、B1-5和C1-2)且未解决的丧失/创伤发生率较低的非临床组儿童相比,患有性别焦虑症的儿童大多被归类为高风险依恋模式(A3-4、A5-6、C3-4、C5-6和A/C)(χ = 52.66;<0.001),且未解决的丧失/创伤发生率较高(χ = 18.64;<0.001)。共病精神诊断(= 50;87.7%)以及自伤史、自杀意念或痛苦症状也很常见。整体功能水平受损(范围为25-95/100;平均值 = 54.88;= 15.40;中位数 = 55.00)。患有性别焦虑症的儿童与患有混合精神疾病的儿童在依恋模式(χ = 2.43;= 0.30)以及未解决的丧失和创伤发生率(χ = 0.70;= 0.40)方面没有差异。分析表明,较低的社会经济地位、家庭结构(非传统家庭单位)、ACEs(包括虐待[身体虐待、性虐待、情感虐待、忽视和接触家庭暴力])增加了儿童被归类为高风险依恋模式的可能性。与患有其他形式心理困扰的儿童一样,患有性别焦虑症的儿童处于多种相互作用的风险因素背景下,这些因素包括风险依恋、未解决的丧失/创伤、家庭冲突和家庭凝聚力丧失以及接触多种ACEs。