Llitjos Jean-François, Bredin Swann, Lascarrou Jean-Baptiste, Soumagne Thibaud, Cojocaru Mariana, Leclerc Maxime, Lepetit Arnaud, Gouhier Albin, Charpentier Julien, Piton Gaël, Faron Matthieu, Stoclin Annabelle, Pène Frédéric
3i Department, Team Pulmonary and Systemic Immune Responses During Acute and Chronic Bacterial Infections, Institut Cochin, INSERM U1016, CNRS UMR8104, Université de Paris, Paris, France.
Intensive care unit, Gustave Roussy, Université Paris-Saclay, Villejuif, France.
Ann Intensive Care. 2021 Jan 29;11(1):20. doi: 10.1186/s13613-021-00812-w.
The aim of this study is to determine whether severe COVID-19 patients harbour a higher risk of ICU-acquired pneumonia.
This retrospective multicentre cohort study comprised all consecutive patients admitted to seven ICUs for severe COVID-19 pneumonia during the first COVID-19 surge in France. Inclusion criteria were laboratory-confirmed SARS-CoV-2 infection and requirement for invasive mechanical ventilation for 48 h or more. Control groups were two historical cohorts of mechanically ventilated patients admitted to the ICU for bacterial or non-SARS-CoV-2 viral pneumonia. The outcome of interest was the development of ICU-acquired pneumonia. The determinants of ICU-acquired pneumonia were investigated in a multivariate competing risk analysis.
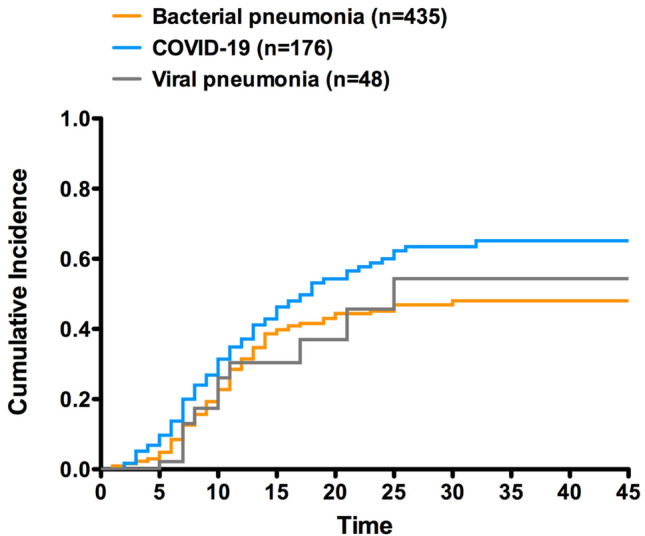
One hundred and seventy-six patients with severe SARS-CoV-2 pneumonia admitted to the ICU between March 1st and 30th June of 2020 were included into the study. Historical control groups comprised 435 patients with bacterial pneumonia and 48 ones with viral pneumonia. ICU-acquired pneumonia occurred in 52% of COVID-19 patients, whereas in 26% and 23% of patients with bacterial or viral pneumonia, respectively (p < 0.001). Times from initiation of mechanical ventilation to ICU-acquired pneumonia were similar across the three groups. In multivariate analysis, the risk of ICU-acquired pneumonia remained independently associated with underlying COVID-19 (SHR = 2.18; 95 CI 1.2-3.98, p = 0.011).
COVID-19 appears an independent risk factor of ICU-acquired pneumonia in mechanically ventilated patients with pneumonia. Whether this is driven by immunomodulatory properties by the SARS-CoV-2 or this is related to particular processes of care remains to be investigated.
本研究旨在确定重症新型冠状病毒肺炎(COVID-19)患者发生重症监护病房(ICU)获得性肺炎的风险是否更高。
这项回顾性多中心队列研究纳入了法国首次COVID-19疫情高峰期间因重症COVID-19肺炎入住7个ICU的所有连续患者。纳入标准为实验室确诊的严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染且需要有创机械通气48小时或更长时间。对照组为因细菌性或非SARS-CoV-2病毒性肺炎入住ICU的两个机械通气患者的历史队列。感兴趣的结局是ICU获得性肺炎的发生。在多变量竞争风险分析中研究了ICU获得性肺炎的决定因素。
2020年3月1日至6月30日期间入住ICU的176例重症SARS-CoV-2肺炎患者纳入研究。历史对照组包括435例细菌性肺炎患者和48例病毒性肺炎患者。52%的COVID-19患者发生了ICU获得性肺炎,而细菌性或病毒性肺炎患者的这一比例分别为26%和23%(p<0.001)。三组从机械通气开始到发生ICU获得性肺炎的时间相似。在多变量分析中,ICU获得性肺炎的风险仍然与潜在的COVID-19独立相关(风险比=2.18;95%置信区间1.2 - 3.98,p = 0.011)。
对于机械通气的肺炎患者,COVID-19似乎是ICU获得性肺炎的独立危险因素。这是由SARS-CoV-2的免疫调节特性驱动还是与特定的护理过程有关,仍有待研究。