Department of Pulmonary Medicine, Erasmus MC Cancer Institute, Doctor Molewaterplein 40, 3015 GD Rotterdam, the Netherlands.
Department of Thoracic Oncology, Netherlands Cancer Institute, Amsterdam, the Netherlands.
EBioMedicine. 2021 Feb;64:103160. doi: 10.1016/j.ebiom.2020.103160. Epub 2021 Jan 27.
Gemcitabine is a frequently used chemotherapeutic agent but its effects on the immune system are incompletely understood. Recently, the randomized NVALT19-trial revealed that maintenance gemcitabine after first-line chemotherapy significantly prolonged progression-free survival (PFS) compared to best supportive care (BSC) in malignant mesothelioma. Whether these effects are paralleled by changes in circulating immune cell subsets is currently unknown. These analyses could offer improved mechanistic insights into the effects of gemcitabine on the host and guide development of effective combination therapies in mesothelioma.
We stained peripheral blood mononuclear cells (PBMCs) and myeloid-derived suppressor cells (MDSCs) at baseline and 3 weeks following start of gemcitabine or BSC treatment in a subgroup of mesothelioma patients included in the NVALT19-trial. In total, 24 paired samples including both MDSCs and PBMCs were included. We performed multicolour flow-cytometry to assess co-inhibitory and-stimulatory receptor- and cytokine expression and matched these parameters with PFS and OS.
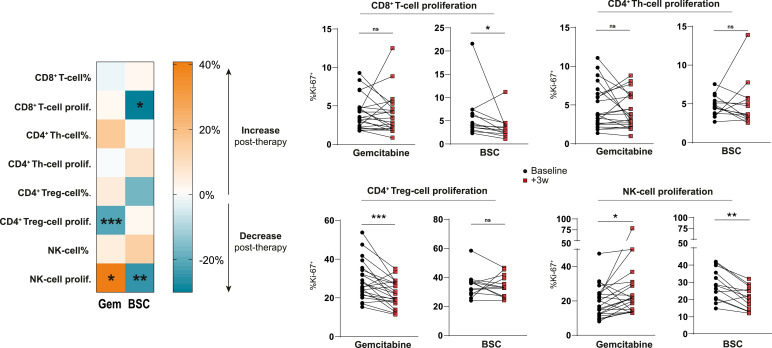
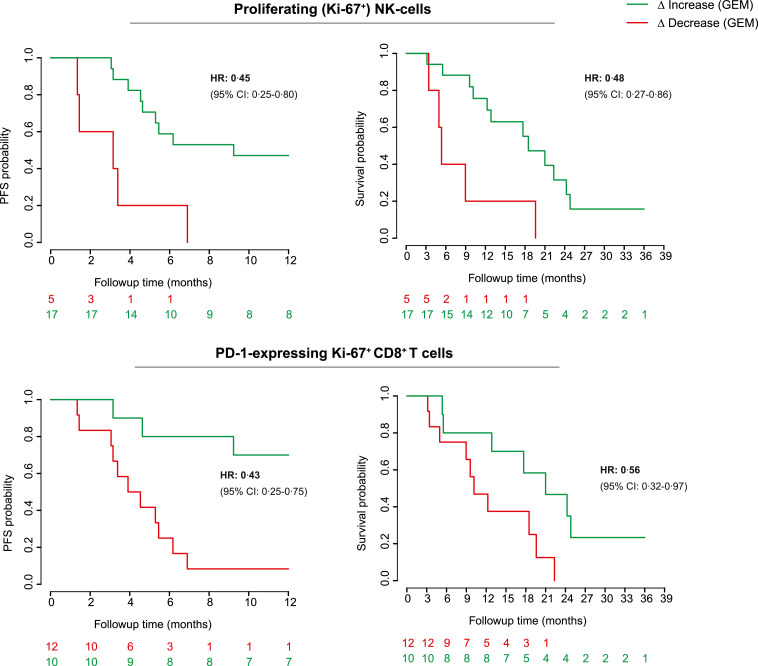
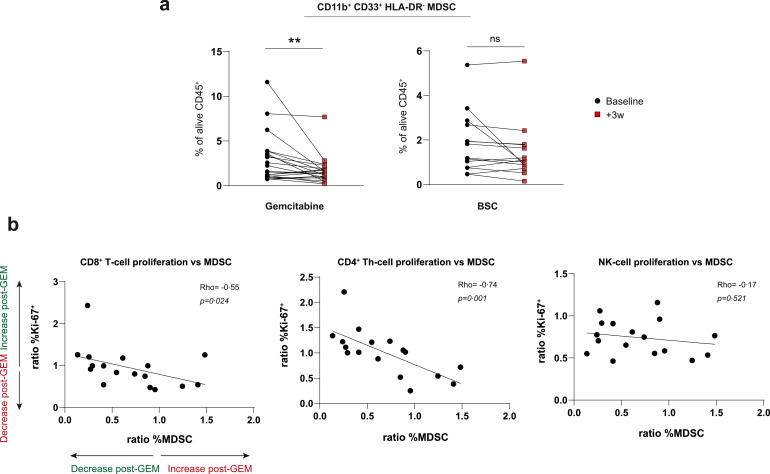
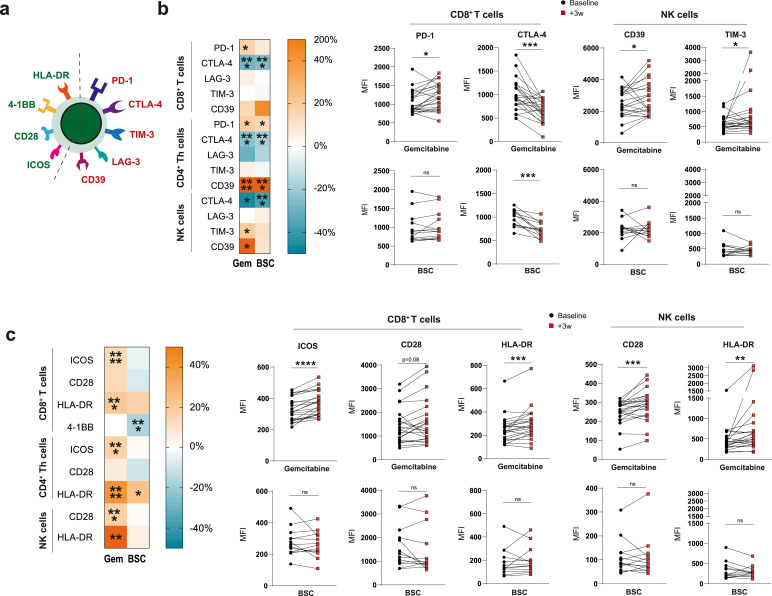
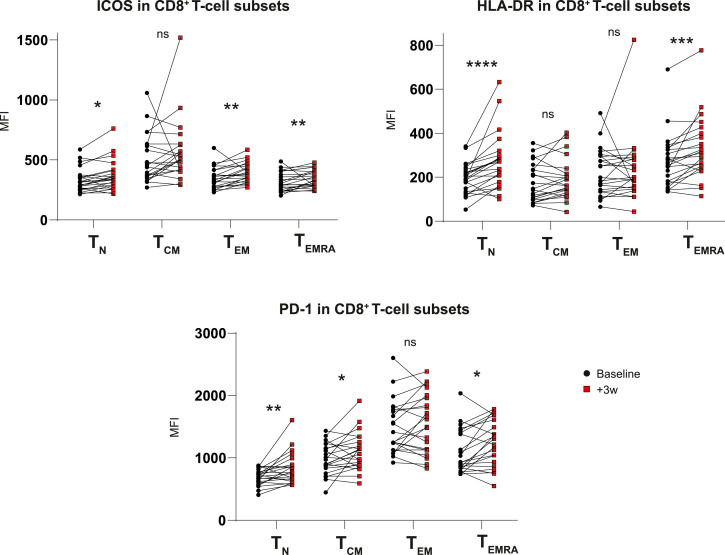
Gemcitabine treatment was significantly associated with an increased NK-cell- and decreased T-regulatory cell proliferation whereas the opposite occurred in control patients. Furthermore, myeloid-derived suppressor cells (MDSCs) frequencies were lower in gemcitabine-treated patients and this correlated with increased T-cell proliferation following treatment. Whereas gemcitabine variably altered co-inhibitory receptor expression, co-stimulatory molecules including ICOS, CD28 and HLA-DR were uniformly increased across CD4 T-helper, CD8 T- and NK-cells. Although preliminary in nature, the increase in NK-cell proliferation and PD-1 expression in T cells following gemcitabine treatment was associated with improved PFS and OS.
Gemcitabine treatment was associated with widespread effects on circulating immune cells of mesothelioma patients with responding patients displaying increased NK-cell and PD-1 + T-cell proliferation. These exploratory data provide a platform for future on treatment-biomarker development and novel combination treatment strategies.
吉西他滨是一种常用的化疗药物,但它对免疫系统的影响尚未完全阐明。最近,随机 NVALT19 试验显示,与最佳支持治疗(BSC)相比,一线化疗后维持吉西他滨治疗可显著延长恶性间皮瘤患者的无进展生存期(PFS)。目前尚不清楚这些影响是否与循环免疫细胞亚群的变化平行。这些分析可以为吉西他滨对宿主的影响提供更好的机制见解,并指导间皮瘤中有效联合治疗的发展。
我们在 NVALT19 试验中纳入的间皮瘤患者亚组中,在开始吉西他滨或 BSC 治疗的第 3 周时,对患者的外周血单核细胞(PBMC)和髓系来源的抑制细胞(MDSC)进行染色。总共纳入了 24 对包括 MDSC 和 PBMC 的样本。我们进行了多色流式细胞术评估共抑制和共刺激受体和细胞因子表达,并将这些参数与 PFS 和 OS 进行了匹配。
吉西他滨治疗与 NK 细胞增殖增加和 T 调节细胞增殖减少显著相关,而对照组患者则相反。此外,吉西他滨治疗患者的髓系来源的抑制细胞(MDSC)频率较低,并且这与治疗后 T 细胞增殖增加相关。尽管吉西他滨改变了共抑制受体的表达,但共刺激分子,包括 ICOS、CD28 和 HLA-DR,在 CD4 T 辅助细胞、CD8 T 细胞和 NK 细胞中均增加。虽然性质初步,但吉西他滨治疗后 NK 细胞增殖和 T 细胞中 PD-1 表达的增加与 PFS 和 OS 的改善相关。
吉西他滨治疗与间皮瘤患者循环免疫细胞的广泛影响相关,有反应的患者显示 NK 细胞和 PD-1+T 细胞增殖增加。这些探索性数据为未来的治疗生物标志物开发和新型联合治疗策略提供了一个平台。