Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine; Center for Hyperbaric Medicine and Environmental Physiology, Department of Anesthesiology, Duke University School of Medicine, Durham, North Carolina.
Division of Pulmonary, Allergy, and Critical Care Medicine, Department of Medicine.
J Heart Lung Transplant. 2021 Apr;40(4):269-278. doi: 10.1016/j.healun.2021.01.008. Epub 2021 Jan 15.
Central airway stenosis (CAS) is a severe airway complication after lung transplantation associated with bronchial ischemia and necrosis. We sought to determine whether hyperbaric oxygen therapy (HBOT), an established treatment for tissue ischemia, attenuates post-transplant bronchial injury.
We performed a randomized, controlled trial comparing usual care with HBOT (2 atm absolute for 2 hours × 20 sessions) in subjects with extensive airway necrosis 4 weeks after transplantation. Endobronchial biopsies were collected at 4, 7, and 10 weeks after transplantation for a quantitative polymerase chain reaction. Coprimary outcomes were incidence of airway stenting and acute cellular rejection (ACR) at 1 year.
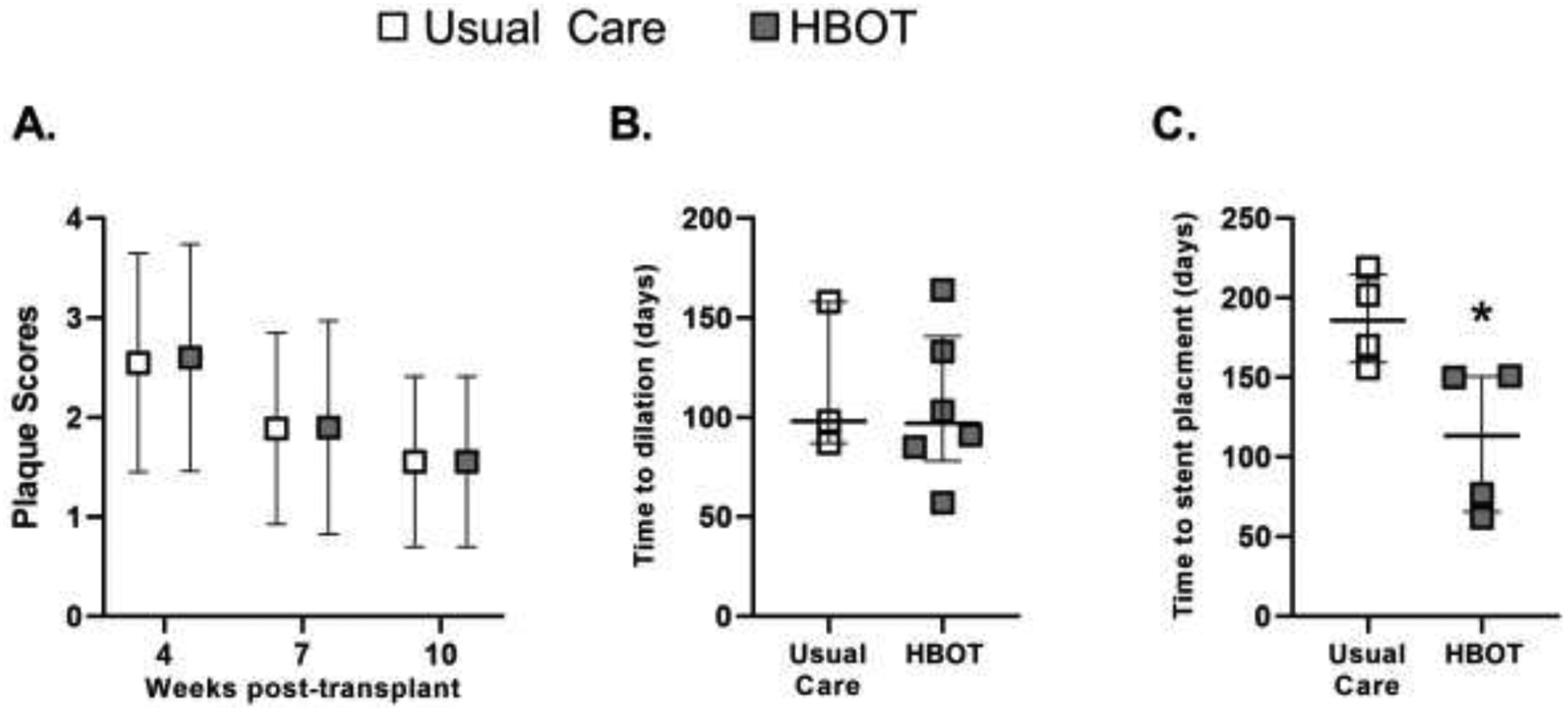
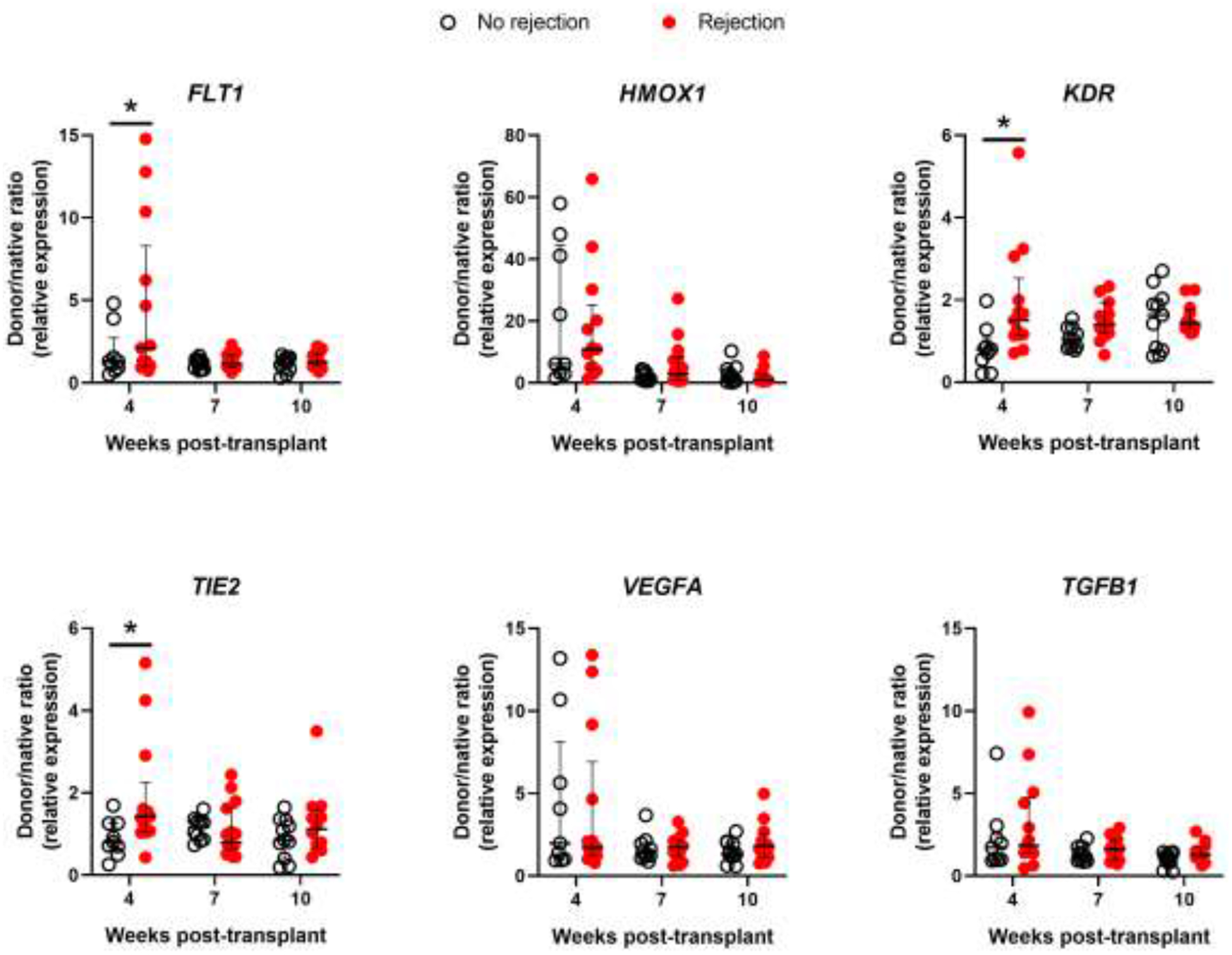
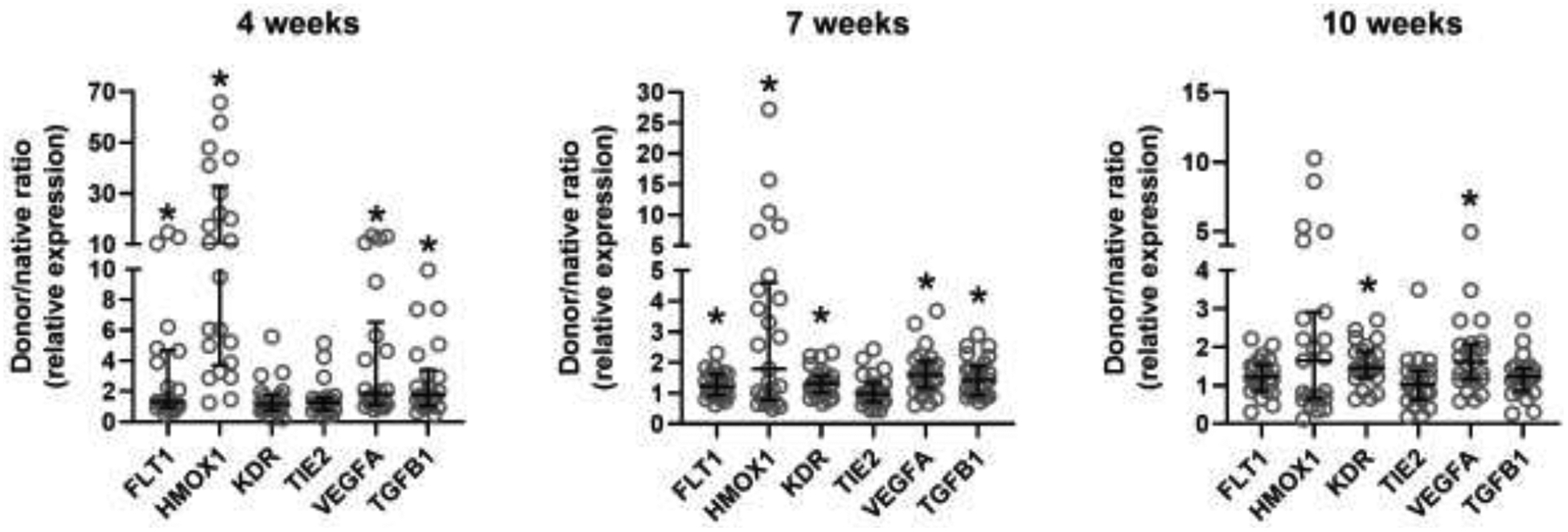
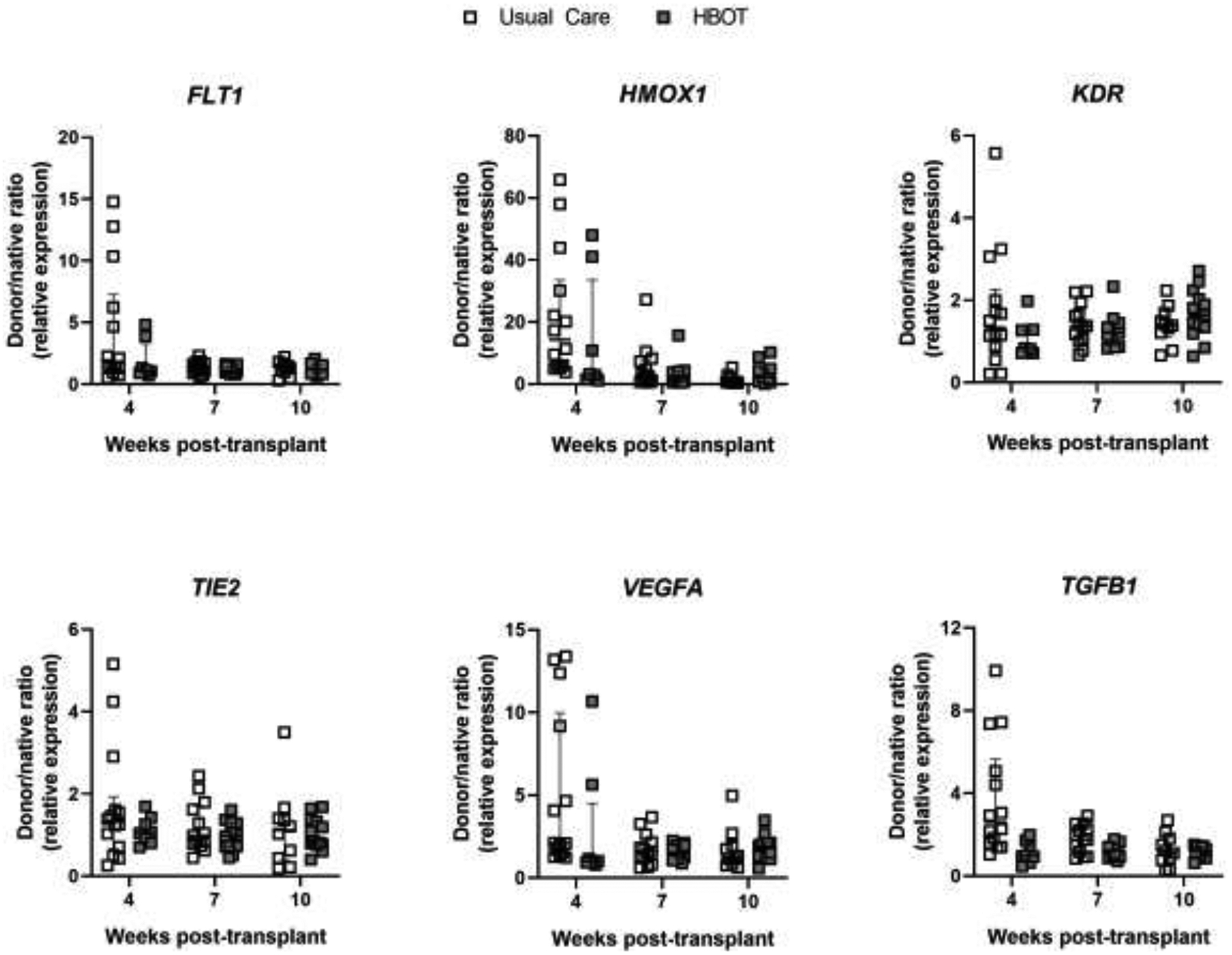
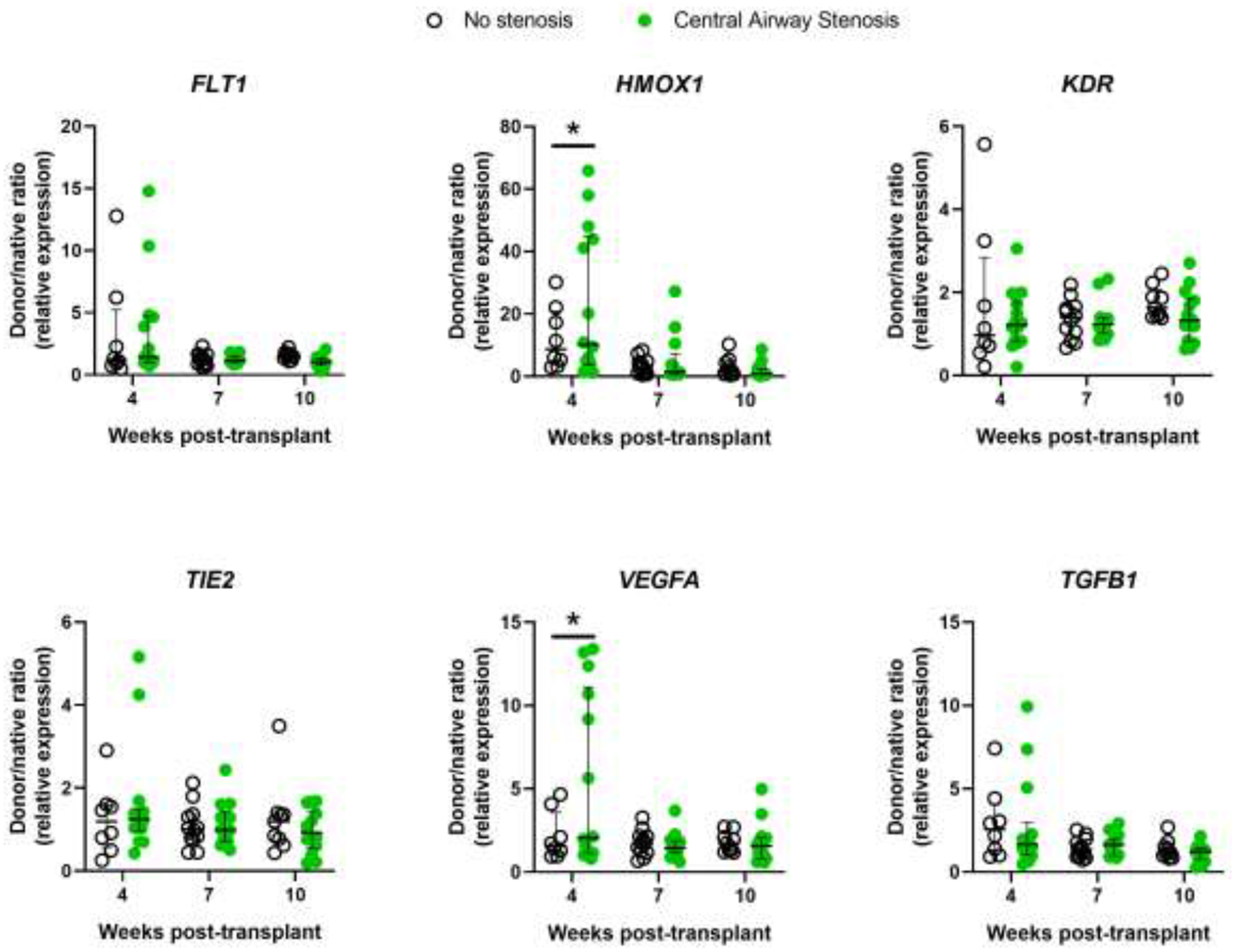
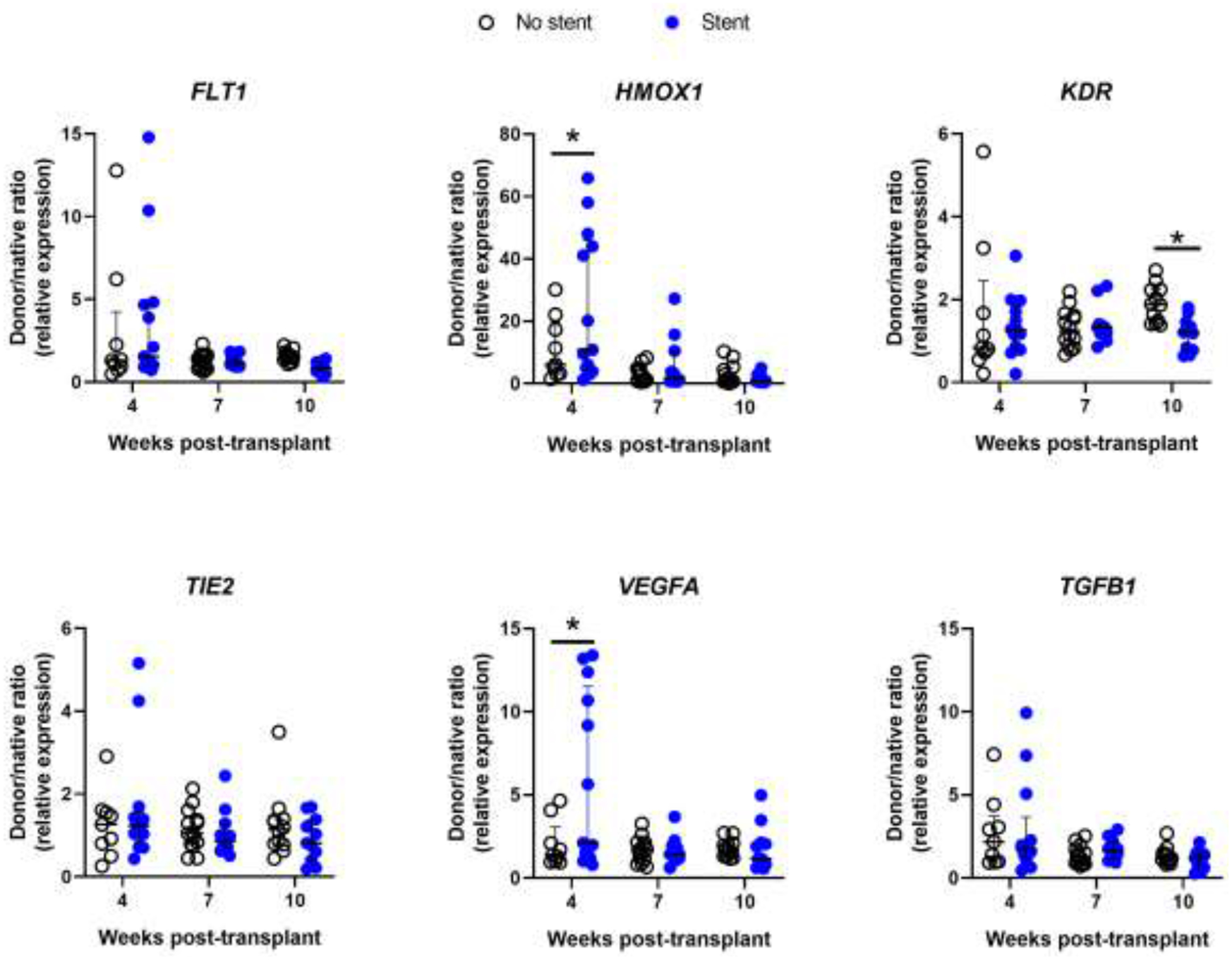
The trial was stopped after enrolling 20 subjects (n = 10 per group) after a pre-planned interim analysis showed no difference between usual care and HBOT groups in stenting (both 40%), ACR (70% and 40%, respectively), or CAS (40% and 60%, respectively). Time to first stent placement (median [interquartile range]) was significantly shorter in the HBOT group (150 [73-150] vs 186 [167-206] days, p < 0.05). HIF gene expression was significantly increased in donor tissues at 4, 7, and 10 weeks after transplantation but was not altered by HBOT. Subjects who developed CAS or required stenting had significantly higher HMOX1 and VEGFA expression at 4 weeks (both p < 0.05). Subjects who developed ACR had significant FLT1, TIE2, and KDR expression at 4 weeks (all p < 0.05).
Incidence of CAS is high after severe, established airway necrosis after transplantation. HBOT does not reduce CAS severity or stenting. Elevated HMOX1 and VEGFA expressions appear to associate with airway complications.
中心气道狭窄(CAS)是肺移植后严重的气道并发症,与支气管缺血和坏死有关。我们试图确定高压氧治疗(HBOT)是否能减轻移植后的支气管损伤,因为它是一种治疗组织缺血的既定方法。
我们进行了一项随机对照试验,比较了广泛气道坏死发生在移植后 4 周时的常规治疗与 HBOT(2 个大气压绝对压力,2 小时×20 次)的疗效。在移植后 4、7 和 10 周时,通过定量聚合酶链反应收集支气管内活检标本。主要终点是 1 年内气道支架置入和急性细胞排斥反应(ACR)的发生率。
在计划中的中期分析显示常规治疗和 HBOT 组在支架置入(分别为 40%和 70%和 40%)、ACR(分别为 40%和 40%)或 CAS(分别为 40%和 60%)方面没有差异后,试验在纳入 20 名受试者(每组 10 名)后停止。HBOT 组首次支架放置的时间(中位数[四分位数范围])明显短于常规治疗组(150[73-150]与 186[167-206]天,p<0.05)。在移植后 4、7 和 10 周时,供体组织中的 HIF 基因表达明显增加,但 HBOT 并未改变其表达。发生 CAS 或需要支架置入的患者在 4 周时的 HMOX1 和 VEGFA 表达明显升高(均 p<0.05)。发生 ACR 的患者在 4 周时的 FLT1、TIE2 和 KDR 表达明显升高(均 p<0.05)。
在严重的、已确立的气道坏死发生后,移植后 CAS 的发生率很高。HBOT 不能降低 CAS 的严重程度或支架置入率。升高的 HMOX1 和 VEGFA 表达似乎与气道并发症有关。