Quisisana Hospital, Ferrara.
Acta Biomed. 2020 Nov 10;91(4):e2020164. doi: 10.23750/abm.v91i4.10540.
There is a scarcity of data regarding the effect of hypertension on the clinical presentation and outcome of symptomatic patients with COVID-19 infection in comparison with non-hypertensive patients.
To describe the clinical presentation, radiological and hematological data of a cohort of symptomatic COVID-19 positive hypertensive patients (n=50) in comparison with another cohort of normotensive symptomatic COVID-19 positive patients (n=250) diagnosed at the same time and managed in the same health facilities (from Jan 2020 to May 2020). Associated comorbidities were assessed, and the Charlson Comorbidity Index was calculated. The outcomes, including duration of hospitalization, length of ICU stay, duration of mechanical ventilation, and duration of O2 supplementation, were also assessed.
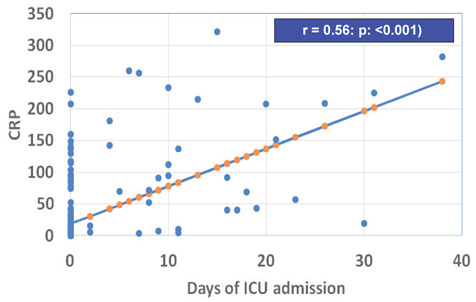
The prevalence of hypertension in symptomatic COVID-19 positive patients was 50/300 (16%; the prevalence of hypertension in Qatari adults is ~30%). Hypertensive patients had a higher prevalence of DM, CKD, and cardiac dysfunction compared to normotensive patients (p<0.01).They had a higher Charlson Co-morbidity score (2.3±1.8) compared to the normotensive patients (0.4±0.9) (p<0.01). Clinically and radiologically, hypertensive patients had significantly higher percentage of pneumonia, severe pneumonia, and ARDS versus normotensive patients (p<0.01). CBC and differential WBC did not differ between hypertensive and normotensive patients. Hypertensive patients had significantly higher CRP(58.5±84), compared to normotensive patients (28±59) (p<0.01). Furthermore, a longer duration of hospitalization, intensive care unit (ICU) stay, mechanical ventilation and oxygen therapy versus normotensive patients was also observed. CRP was correlated significantly with the duration of stay in the ICU and the duration for oxygen supplementation (r=0.56 and 0.61, respectively; p<0.01).
Hypertensive patients with COVID-19 had a higher inflammatory response (higher CRP levels), a significant increase of comorbidities, and a more aggressive course of the disease necessitating a higher rate of ICU admission, longer requirement for hospitalization and oxygen use compared to normotensive patients.
与非高血压患者相比,高血压对 COVID-19 感染有症状患者的临床表现和结局的影响的数据很少。
描述一组同时在同一医疗机构诊断出的患有 COVID-19 的有症状高血压阳性患者(n=50)与另一组患有 COVID-19 的有症状正常血压阳性患者(n=250)的临床症状、影像学和血液学数据。评估相关合并症,并计算 Charlson 合并症指数。还评估了结局,包括住院时间、重症监护病房(ICU)住院时间、机械通气时间和氧气补充时间。
在患有 COVID-19 的有症状阳性患者中,高血压的患病率为 50/300(16%;卡塔尔成年人的高血压患病率约为 30%)。与正常血压患者相比,高血压患者患有糖尿病、慢性肾脏病和心功能障碍的比例更高(p<0.01)。他们的 Charlson 合并症评分(2.3±1.8)高于正常血压患者(0.4±0.9)(p<0.01)。临床和影像学上,高血压患者肺炎、重症肺炎和急性呼吸窘迫综合征的比例明显高于正常血压患者(p<0.01)。高血压和正常血压患者的全血细胞计数和白细胞分类计数无差异。高血压患者的 C 反应蛋白(CRP)明显高于正常血压患者(58.5±84),与正常血压患者(28±59)相比,差异有统计学意义(p<0.01)。此外,高血压患者的住院时间、重症监护病房(ICU)住院时间、机械通气和氧疗时间均明显长于正常血压患者。CRP 与 ICU 住院时间和氧疗时间呈显著正相关(r=0.56 和 0.61,p<0.01)。
与正常血压患者相比,患有 COVID-19 的高血压患者炎症反应更高(CRP 水平更高)、合并症明显增加,且疾病进展更具侵袭性,需要更高的 ICU 入院率、更长的住院时间和氧气使用时间。