Alnafiey Mohammed Obaid, Alangari Abdullah Meshari, Alarifi Abdullah Mohammed, Abushara Ahmed
Department of Internal Medicine, KSMC, Alimam Turki Ibn Abdullah Ibn Muhammed, Ulaishah, Riyadh, 12746, Saudi Arabia.
Saudi Electronic University, P.O.Box: 32109, Riyadh, 11428, Saudi Arabia.
Ann Med Surg (Lond). 2021 Feb;62:358-361. doi: 10.1016/j.amsu.2021.01.049. Epub 2021 Jan 27.
SARS-CoV-2 is a novel infection that has affected millions of people around the world. Complications of the infection may affect multiple systems including cardiovascular, neurological, gastrointestinal, urinary, and pulmonary systems. Hypokalemia, which is a life-threatening condition that may lead to arrhythmia and possibly death, has been noticed in more than half of the COVID-19 patients. Further understanding of the disease process and its complications is necessary to guide in preventing the complications from happening in the first place and finding treatment for patients with an already established complications.
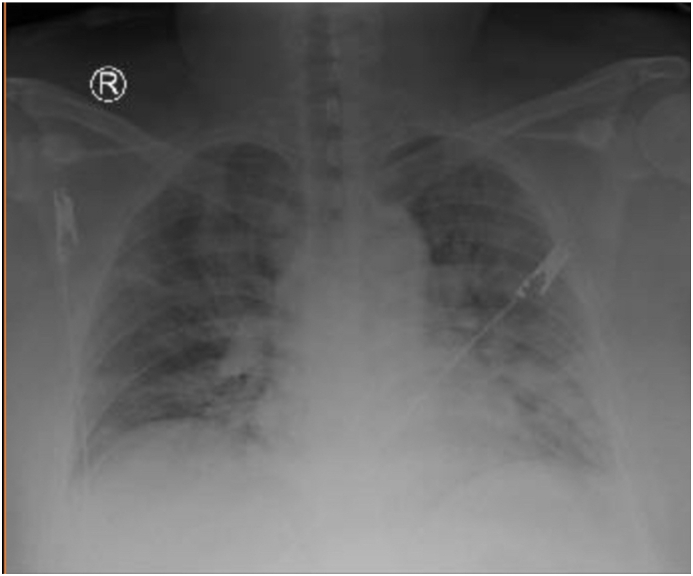
A 34-year old male from Philippines who lives in Saudi Arabia - Riyadh and works as health care provider with no previous history of any medical illness. Presented by himself to the emergency department (ED) with dry cough, shortness of breath, fever, malaise, and fatigability for five days. On examination (RR 25), (T 38.6 °C) and (O2 89% Room air), on auscultation there was a decrease on air entry bilaterally with scattered crepitations, no wheezing or stridor. Covid-19 swab was positive, (Day 1) potassium 2.91 (mmol/L) magnesium (mmol/L) with normal baseline before getting infected.
Patient while in the hospital was on daily potassium oral and IV replacement with IV magnesium replacement. Investigation showed 24Hr urine potassium 47.3 (mmol/L), 24Hr urine magnesium 5.52 (mmol/L), 24Hr urine Creatinine 9.25 (mmol/L), (TTKG) Transtubular Potassium Gradient 18 and (VBG) PH:7.38, Pco2:44 (mmHg) Po2:55 (mmHg) HCO3:25 (mEq/L). Patient has an increased renal potassium loss with normal VBG on separate days and normal Blood pressure that excludes diseases with associated acidemia or alkalemia. Our patient didn't want to go for any invasive diagnostic procedures and favored to wait for spontaneous recovery.
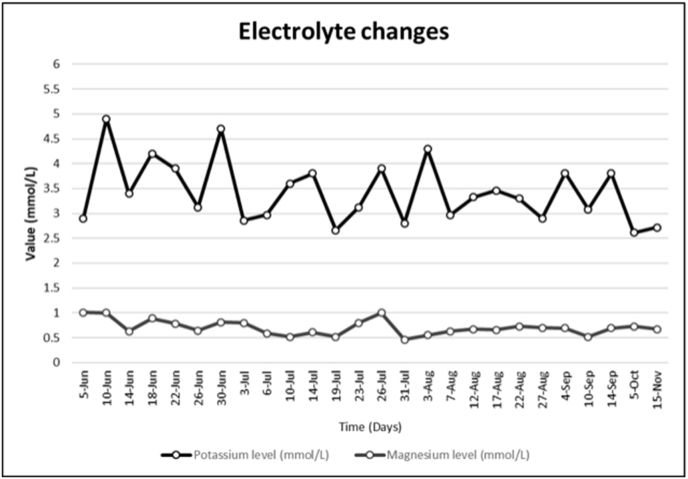
We followed up the potassium level of our patient for more than 5 months since he was diagnosed with COVID-19 to find out that he is still having hypokalemia, as well as, hypomagnesemia. Long term complications of COVID-19 infection such as hypokalemia and hypomagnesemia need to be observed and followed up closely to avoid life-threatening arrythmias and seizures. The attention of the scientific community to possible long term or permanent complications is needed to help find preventive measures and treatment for patients with complications.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)是一种新型感染源,已影响全球数百万人。该感染的并发症可能累及多个系统,包括心血管系统、神经系统、胃肠道、泌尿系统和肺部系统。低钾血症是一种危及生命的状况,可能导致心律失常甚至死亡,在超过半数的2019冠状病毒病(COVID-19)患者中都有发现。进一步了解该疾病的进程及其并发症,对于首先预防并发症的发生以及为已经出现并发症的患者寻找治疗方法至关重要。
一名34岁男性,来自菲律宾,居住在沙特阿拉伯利雅得,从事医疗保健工作,既往无任何病史。因干咳、气短、发热、乏力和疲倦五天,自行前往急诊科就诊。体格检查显示(呼吸频率25次/分钟),(体温38.6摄氏度),(室内空气中氧饱和度89%),听诊双肺呼吸音减弱,可闻及散在湿啰音,无哮鸣音或喘鸣音。新冠病毒拭子检测呈阳性,(第1天)血钾2.91(毫摩尔/升),血镁(毫摩尔/升),感染前基线正常。
患者住院期间每日口服及静脉补钾,并静脉补充镁。检查显示24小时尿钾47.3(毫摩尔/升),24小时尿镁5.52(毫摩尔/升),24小时尿肌酐9.25(毫摩尔/升),肾小管钾梯度(TTKG)为18,静脉血气分析(VBG)显示pH值:7.38,二氧化碳分压:44(毫米汞柱),氧分压:55(毫米汞柱),碳酸氢根:25(毫当量/升)。患者存在肾性钾丢失增加,不同日期的静脉血气分析结果正常,血压正常,可排除伴有酸血症或碱血症的疾病。我们的患者不愿接受任何侵入性诊断检查,希望等待自然康复。
自该患者被诊断为COVID-19以来,我们对其血钾水平进行了5个多月的随访,发现他仍患有低钾血症以及低镁血症。COVID-19感染的长期并发症,如低钾血症和低镁血症,需要密切观察和随访,以避免危及生命的心律失常和癫痫发作。科学界需要关注可能的长期或永久性并发症,以帮助找到针对并发症患者的预防措施和治疗方法。