Stroke Research Group, Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK.
Department of Psychology, King's College London, London, UK.
Int J Stroke. 2021 Jul;16(5):510-518. doi: 10.1177/1747493021990906. Epub 2021 Feb 4.
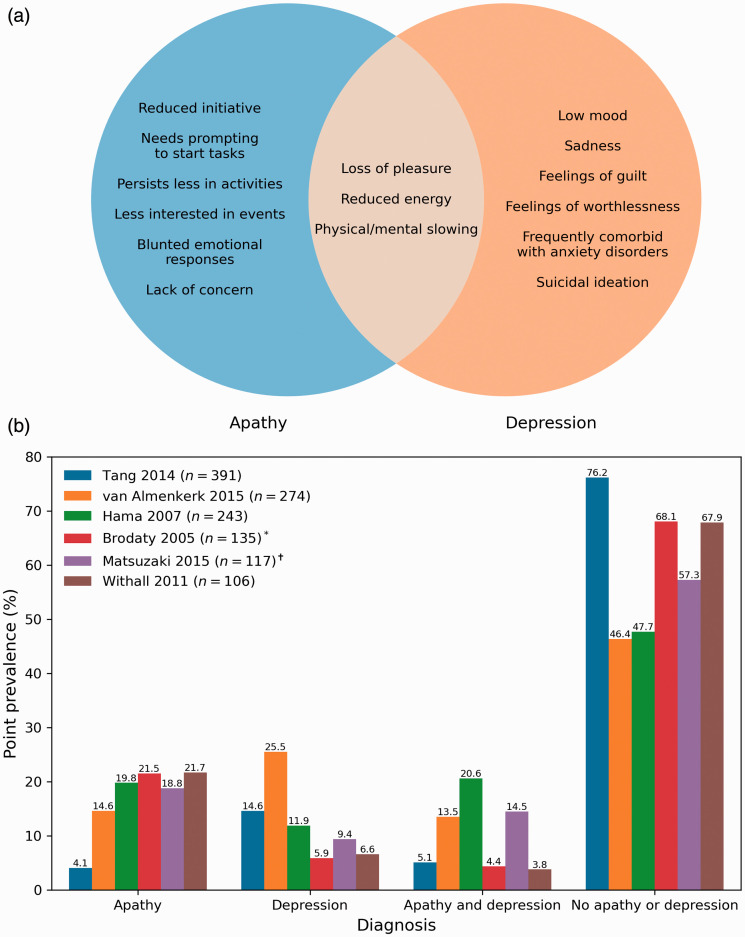
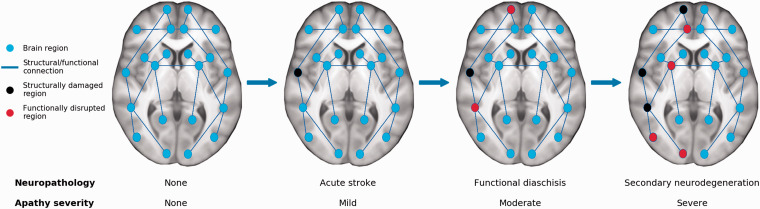
Apathy is a reduction in goal-directed activity in the cognitive, behavioral, emotional, or social domains of a patient's life and occurs in one out of three patients after stroke. Despite this, apathy is clinically under-recognized and poorly understood. This overview provides a contemporary introduction to apathy in stroke for researchers and practitioners, covering topics including diagnosis, neurobiological mechanisms, associated consequences, and potential treatments for apathy. Apathy is often misdiagnosed as other post-stroke conditions such as depression. Accurate differential diagnosis of apathy, which manifests as reductions in initiative, and depression, which manifests as negative emotionality, is important as it informs prognosis. Research on the neurobiology of apathy suggests that there are few consistent associations between stroke lesion location and the development of apathy. These may be resolved by adopting a network neuroscience approach, which models apathy as a pathology arising from structural or functional damage to brain networks underlying motivated behavior. Importantly, networks can be affected by physiological changes related to stroke, including the acute infarct but also diaschisis and neurodegeneration. Aside from neurobiological changes, apathy is also associated with other negative outcome measures such as functional disability, cognitive impairment, and emotional distress, suggesting that apathy is indicative of a worse prognosis following stroke. Unfortunately, high-quality trials aimed at treating apathy are scarce. Antidepressants may have limited effects on apathy. Acetylcholine and dopamine pharmacotherapy, behavioral interventions, and transcranial magnetic stimulation may be more promising avenues for treatment.
淡漠是指患者生活中的认知、行为、情感或社交领域中目标导向活动的减少,三分之一的中风患者会出现这种情况。尽管如此,淡漠在临床上仍未得到充分认识和理解。本篇综述为研究人员和从业者提供了中风后淡漠的当代概述,涵盖了诊断、神经生物学机制、相关后果以及淡漠的潜在治疗方法等主题。淡漠常常被误诊为其他中风后的病症,如抑郁症。准确地区分淡漠和抑郁症的诊断非常重要,因为这可以为预后提供信息。淡漠的表现为主动性降低,而抑郁症的表现为负性情绪,准确地区分淡漠和抑郁症非常重要。对淡漠的神经生物学研究表明,中风后发生淡漠与脑损伤部位之间的关联很少有一致性。通过采用网络神经科学方法,将淡漠建模为与动机行为相关的大脑网络的结构或功能损伤引起的病理学,可能可以解决这个问题。重要的是,网络可能会受到与中风相关的生理变化的影响,包括急性梗死,还包括远隔区和神经退行性变。除了神经生物学变化,淡漠还与其他负面结果测量指标相关,如功能障碍、认知障碍和情绪困扰,这表明淡漠是中风后预后较差的一个指标。不幸的是,旨在治疗淡漠的高质量试验很少。抗抑郁药可能对淡漠的治疗效果有限。乙酰胆碱和多巴胺药物治疗、行为干预和经颅磁刺激可能是更有前途的治疗方法。