Wang Pengfei, Liu Lihong, Iketani Sho, Luo Yang, Guo Yicheng, Wang Maple, Yu Jian, Zhang Baoshan, Kwong Peter D, Graham Barney S, Mascola John R, Chang Jennifer Y, Yin Michael T, Sobieszczyk Magdalena, Kyratsous Christos A, Shapiro Lawrence, Sheng Zizhang, Nair Manoj S, Huang Yaoxing, Ho David D
Aaron Diamond AIDS Research Center, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, USA.
Department of Microbiology and Immunology, Columbia University Irving Medical Center, New York, NY, USA.
Res Sq. 2021 Jan 29:rs.3.rs-155394. doi: 10.21203/rs.3.rs-155394/v1.
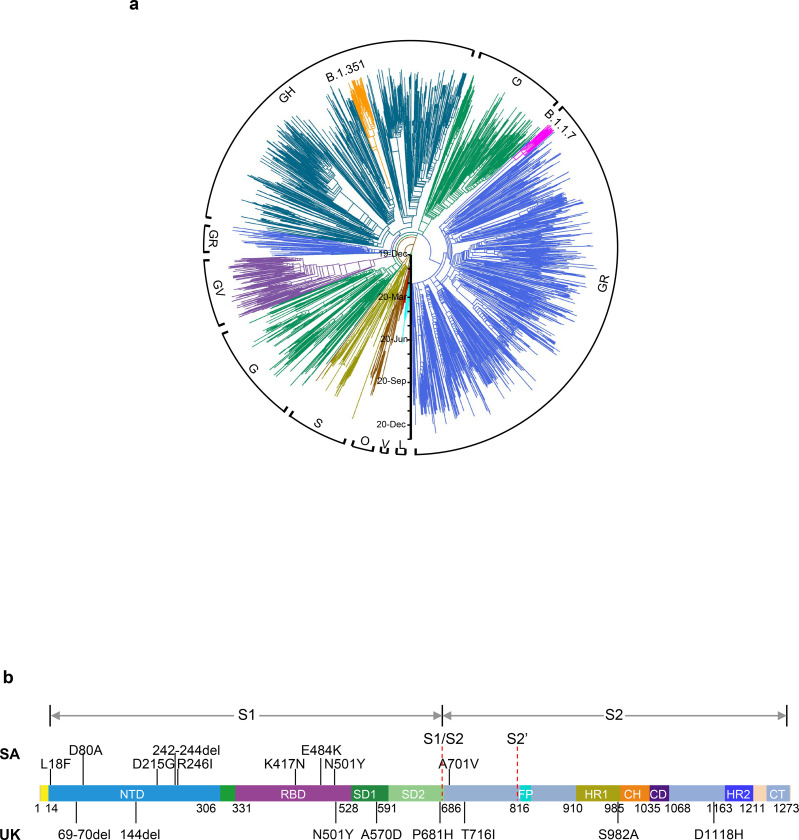
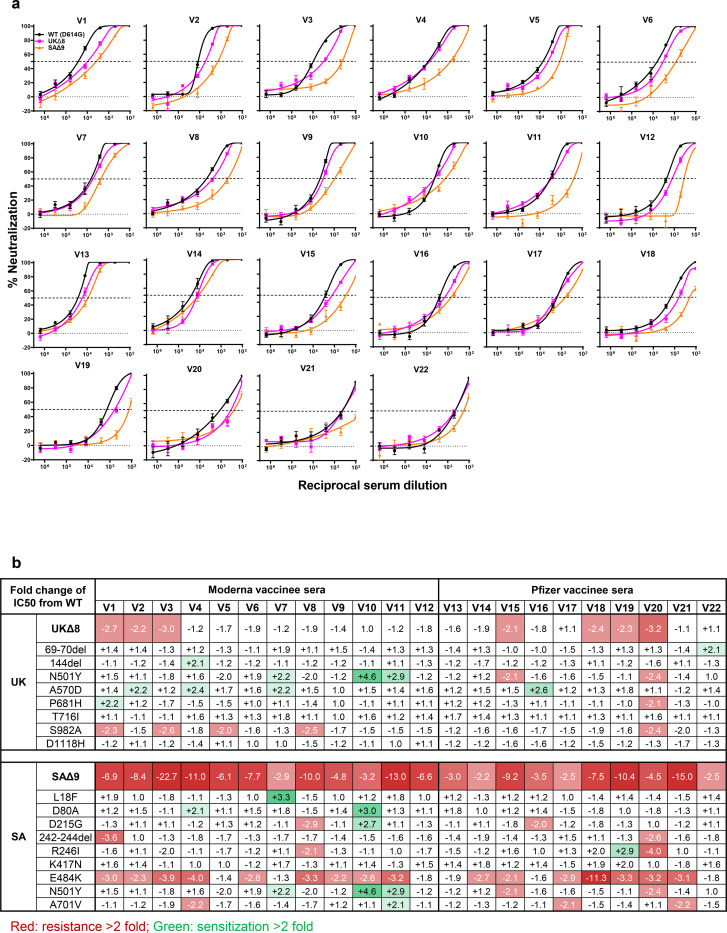
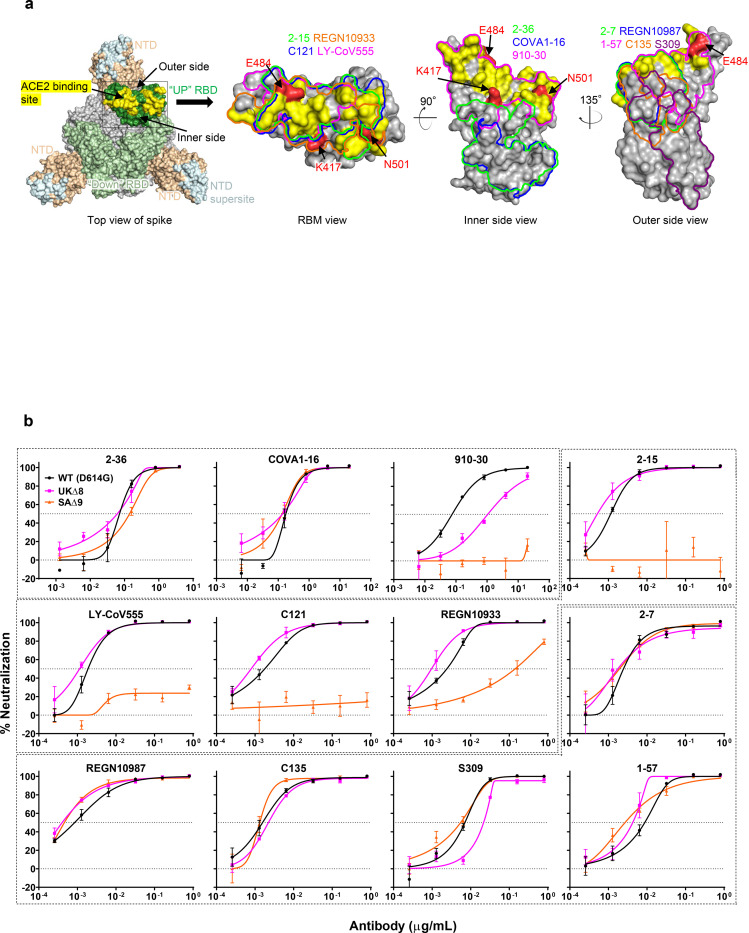
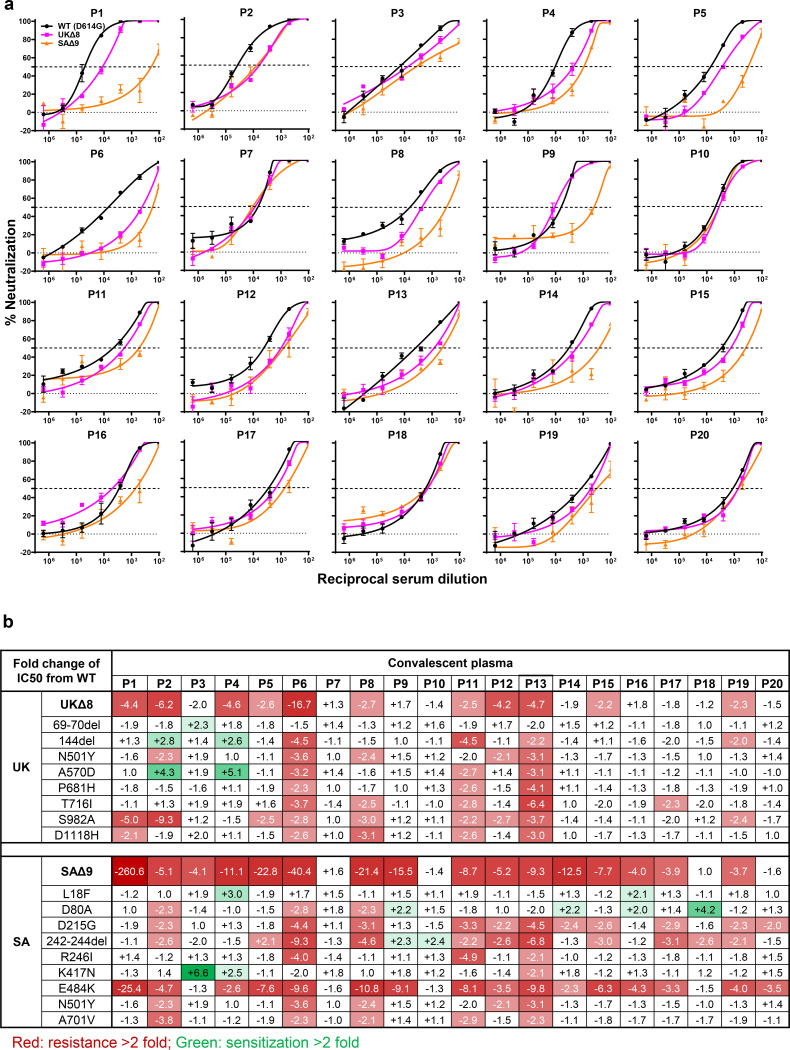
The Covid-19 pandemic has ravaged the globe, and its causative agent, SARS-CoV-2, continues to rage. Prospects of ending this pandemic rest on the development of effective interventions. Two monoclonal antibody (mAb) therapeutics have received emergency use authorization, and more are in the pipeline. Furthermore, multiple vaccine constructs have shown promise, including two with 95% protective efficacy against Covid-19. However, these interventions were directed toward the initial SARS-CoV-2 that emerged in 2019. Considerable viral evolution has occurred since, including variants with a D614G mutation that have become dominant. Viruses with this mutation alone do not appear to be antigenically distinct, however. Recent emergence of new SARS-CoV-2 variants B.1.1.7 in the UK and B.1.351 in South Africa is of concern because of their purported ease of transmission and extensive mutations in the spike protein. We now report that B.1.1.7 is refractory to neutralization by most mAbs to the N-terminal domain (NTD) of spike and relatively resistant to a number of mAbs to the receptor-binding domain (RBD). It is modestly more resistant to convalescent plasma (3 fold) and vaccinee sera (2 fold). Findings on B.1.351 are more worrisome in that this variant is not only refractory to neutralization by most NTD mAbs but also by multiple potent mAbs to the receptor-binding motif on RBD, largely due to an E484K mutation. Moreover, B.1.351 is markedly more resistant to neutralization by convalescent plasma (11-33 fold) and vaccinee sera (~6.5-8.6 fold). B.1.351 and emergent variants with similar spike mutations present new challenges for mAb therapy and threaten the protective efficacy of current vaccines.
新冠疫情肆虐全球,其病原体严重急性呼吸综合征冠状病毒2(SARS-CoV-2)仍在猖獗传播。终结这场疫情的希望寄托在有效干预措施的研发上。两种单克隆抗体(mAb)疗法已获得紧急使用授权,还有更多疗法正在研发中。此外,多种疫苗构建体已显示出前景,其中两种对新冠病毒的保护效力约为95%。然而,这些干预措施针对的是2019年出现的最初的SARS-CoV-2。自那时以来,病毒发生了相当大的进化,包括携带D614G突变的变体已成为主导。然而,仅携带这种突变的病毒在抗原性上似乎并无明显差异。英国出现的新型SARS-CoV-2变体B.1.1.7和南非出现的B.1.351令人担忧,因为据称它们传播容易,且刺突蛋白存在广泛突变。我们现在报告,B.1.1.7对大多数针对刺突蛋白N端结构域(NTD)的单克隆抗体的中和作用具有抗性,并且对一些针对受体结合结构域(RBD)的单克隆抗体具有相对抗性。它对康复期血浆(约3倍)和接种疫苗者血清(约2倍)的抗性略高。关于B.1.351的研究结果更令人担忧,因为该变体不仅对大多数NTD单克隆抗体的中和作用具有抗性,而且对多种针对RBD上受体结合基序的强效单克隆抗体也具有抗性,这主要是由于E484K突变。此外,B.1.351对康复期血浆(约11 - 33倍)和接种疫苗者血清(约6.5 - 8.6倍)的中和作用具有明显更高的抗性。B.1.351以及具有类似刺突突变的新出现变体给单克隆抗体疗法带来了新挑战,并威胁到当前疫苗的保护效力。