Graeser Monika, Schrading Simone, Gluz Oleg, Strobel Kevin, Würstlein Rachel, Kümmel Sherko, Schumacher Claudia, Grischke Eva-Maria, Forstbauer Helmut, Braun Michael, Christgen Matthias, Adams Jascha, Nitzsche Henrik, Just Marianne, Fischer Hans Holger, Aktas Bahriye, Potenberg Jochem, von Schumann Raquel, Kolberg-Liedtke Cornelia, Harbeck Nadia, Kuhl Christiane K, Nitz Ulrike
West German Study Group, Moenchengladbach, Germany.
Ev. Hospital Bethesda, Breast Center Niederrhein, Moenchengladbach, Germany.
Int J Cancer. 2021 May 15;148(10):2614-2627. doi: 10.1002/ijc.33495. Epub 2021 Feb 11.
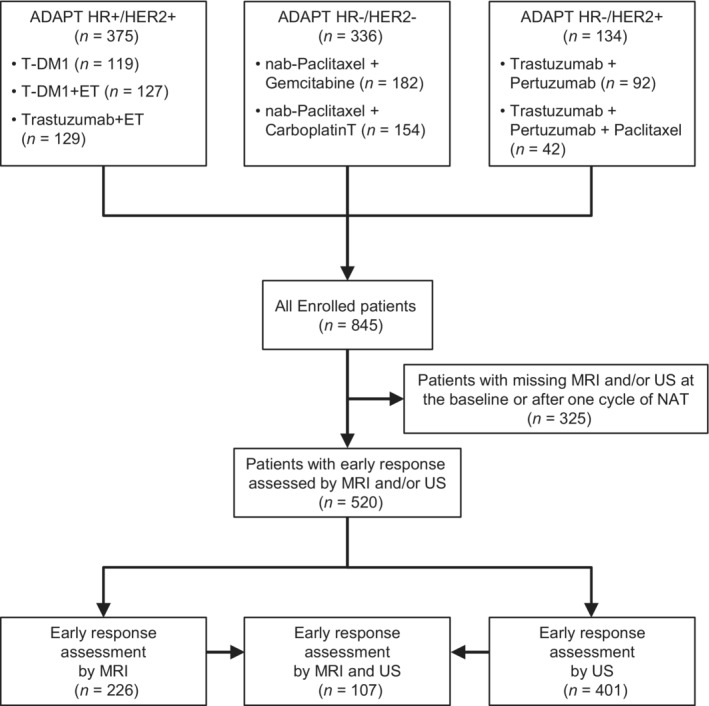
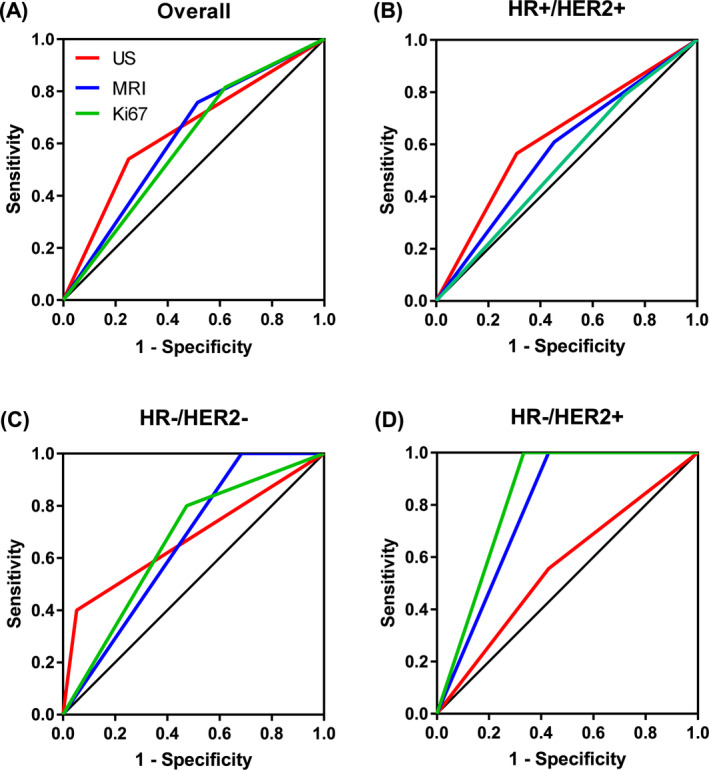
We evaluated the role of early response after 3 weeks of neoadjuvant treatment (NAT) assessed by ultrasound (US), magnetic resonance imaging (MRI) and Ki-67 dynamics for prediction of pathologic complete response (pCR) in different early breast cancer subtypes. Patients with HR+/HER2+, HR-/HER2- and HR-/HER2+ tumors enrolled into three neoadjuvant WSG ADAPT subtrials underwent US, MRI and Ki-67 assessment at diagnosis and after 3 weeks of NAT. Early response was defined as complete or partial response (US, MRI) and ≥30% proliferation decrease or <500 invasive tumor cells (Ki-67). Predictive values and area under the receiver operating characteristic (AUC) curves for prediction of pCR (ypT0/is ypN0) after 12-week NAT were calculated. Two hundred twenty-six had MRI and 401 US; 107 underwent both MRI and US. All three methods yielded a similar AUC in HR+/HER2+ (0.66-0.67) and HR-/HER2- tumors (0.53-0.63), while MRI and Ki-67 performed better than US in HR-/HER2+ tumors (0.83 and 0.79 vs 0.56). Adding MRI+/-Ki-67 increased AUC of US in HR-/HER2+ tumors to 0.64 to 0.75. MRI and Ki-67 demonstrated highest sensitivity in HR-/HER2- (0.8-1) and HR-/HER2+ tumors (1, both). Negative predictive value was similar for all methods in HR+/HER2+ (0.71-0.74) and HR-/HER2- tumors (0.85-1), while it was higher for MRI and Ki-67 compared to US in HR-/HER2+ subtype (1 vs 0.5). Early response assessed by US, MRI and Ki-67 is a strong predictor for pCR after 12-week NAT. Strength of pCR prediction varies according to tumor subtype. Adding MRI+/-Ki-67 to US did not improve pCR prediction in majority of our patients.
我们评估了新辅助治疗(NAT)3周后通过超声(US)、磁共振成像(MRI)和Ki-67动态变化评估的早期反应在预测不同早期乳腺癌亚型病理完全缓解(pCR)中的作用。纳入三项新辅助WSG ADAPT亚试验的HR+/HER2+、HR-/HER2-和HR-/HER2+肿瘤患者在诊断时及NAT 3周后接受了US、MRI和Ki-67评估。早期反应定义为完全或部分反应(US、MRI)以及增殖减少≥30%或浸润性肿瘤细胞<500个(Ki-67)。计算了12周NAT后预测pCR(ypT0/is ypN0)的预测值和受试者操作特征(AUC)曲线下面积。226例患者进行了MRI检查,401例进行了US检查;107例同时接受了MRI和US检查。在HR+/HER2+(0.66 - 0.67)和HR-/HER2-肿瘤(0.53 - 0.63)中,所有三种方法的AUC相似,而在HR-/HER2+肿瘤中,MRI和Ki-67的表现优于US(分别为0.83和0.79,而US为0.56)。在HR-/HER2+肿瘤中,添加MRI±Ki-67可使US的AUC提高到0.64至0.75。MRI和Ki-67在HR-/HER2-(0.8 - 1)和HR-/HER2+肿瘤(两者均为1)中显示出最高的敏感性。在HR+/HER2+(0.71 - 0.74)和HR-/HER2-肿瘤(0.85 - 1)中,所有方法的阴性预测值相似,而在HR-/HER2+亚型中,MRI和Ki-67的阴性预测值高于US(分别为1和0.5)。通过US、MRI和Ki-67评估的早期反应是12周NAT后pCR的有力预测指标。pCR预测的强度因肿瘤亚型而异。在我们的大多数患者中,将MRI±Ki-67添加到US中并不能改善pCR预测。