Department of Urology, Seoul National University Bundang Hospital, 82 Gumi-Ro, 173 Beon-gil, Bundang-gu, Seongnam-si, Gyeonggi-do, 13620, South Korea.
Biochemistry, College of Arts and Sciences, Boston College, Newton, MA, USA.
Sci Rep. 2021 Feb 3;11(1):2919. doi: 10.1038/s41598-021-82700-8.
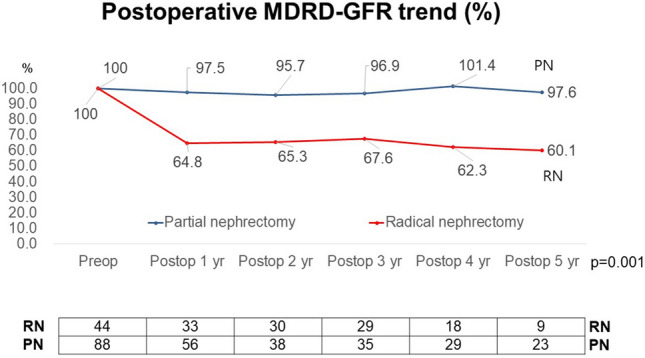
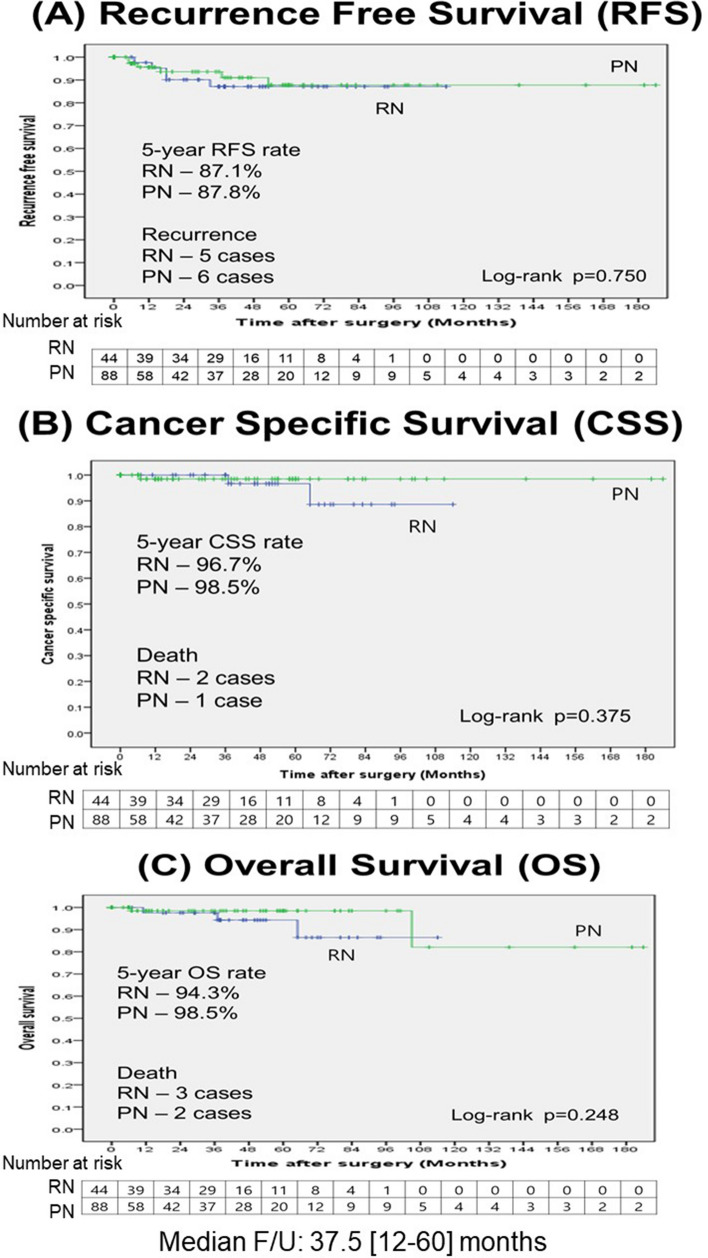
We evaluated the recurrence after radical and partial nephrectomy in patients with RENAL nephrometry score [RENAL] ≥ 10. A total of 474 patients (radical nephrectomy [RN, n = 236] & partial nephrectomy [PN, n = 238]) in a single tertiary referral institution from December 2003 to December 2019 were assessed. Functional outcomes, defined as estimated glomerular filtration rate changes, relapse pattern, recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) were evaluated using propensity score-matched analysis. The predictors of recurrence and survival were assessed by Cox-regression analysis. 44 patients in the RN group and 88 in the PN group were included without significant differences in preoperative clinical factors after matching. The PN patients achieved significantly higher renal function preservation rates (p < 0.001). There were five recurrences in RN and six in PN. The PN patients revealed 5-year RFS rate (86.8%), 5-year CSS rate (98.5%), and 5-year OS rate (98.5%) comparable to the RN patients (RFS: 88.7% [p = 0.780], CSS: 96.7% [p = 0.375], and OS: 94.3% [p = 0.248]). Patients with a body mass index (BMI) ≥ 23 had lower 5-year RFS rates (85.5%) and OS rates (95.6%) than those with BMI < 23 (RFS: 90.0% [p = 0.195], OS: 100% [p = 0.117]) without significance. The significant predictor of recurrence was the pathologic T stage (hazard ratio [HR] 3.99, 95% confidence [CI] 1.10-14.50, p = 0.036). The significant predictor of death was the R domain of the RENAL (HR 3.80, 95% CI 1.03-14.11, p = 0.046). PN, if technically feasible, could be considered to preserve renal function in patients with RENAL ≥ 10. Nonetheless, PN needs to be implemented with caution in some patients due to the higher potentiality for recurrence and poor survival.
我们评估了 RENAL 评分 [RENAL]≥10 的患者接受根治性肾切除术和部分肾切除术的复发情况。在 2003 年 12 月至 2019 年 12 月期间,我们对来自单一三级转诊机构的 474 名患者(根治性肾切除术 [RN,n=236]和部分肾切除术 [PN,n=238])进行了评估。采用倾向评分匹配分析评估功能结局(定义为估算肾小球滤过率变化)、复发模式、无复发生存率(RFS)、癌症特异性生存率(CSS)和总生存率(OS)。采用 Cox 回归分析评估复发和生存的预测因素。在匹配后,RN 组 44 例患者和 PN 组 88 例患者在术前临床因素方面无显著差异。PN 患者的肾功能保留率明显更高(p<0.001)。RN 组有 5 例复发,PN 组有 6 例复发。PN 患者的 5 年 RFS 率(86.8%)、5 年 CSS 率(98.5%)和 5 年 OS 率(98.5%)与 RN 患者相当(RFS:88.7%[p=0.780],CSS:96.7%[p=0.375],OS:94.3%[p=0.248])。BMI≥23 的患者 5 年 RFS 率(85.5%)和 OS 率(95.6%)均低于 BMI<23 的患者(RFS:90.0%[p=0.195],OS:100%[p=0.117]),但无统计学意义。复发的显著预测因素是病理 T 分期(危险比 [HR]3.99,95%置信区间 [CI]1.10-14.50,p=0.036)。死亡的显著预测因素是 RENAL 的 R 域(HR3.80,95%CI1.03-14.11,p=0.046)。如果技术上可行,PN 可考虑用于保留 RENAL≥10 的患者的肾功能。然而,由于复发和生存较差的可能性较高,PN 在某些患者中需要谨慎实施。