Department of Cardiology, Angiology and Intensive Care, Philipps University Marburg, Marburg, Germany.
J Interv Cardiol. 2021 Jan 18;2021:8843935. doi: 10.1155/2021/8843935. eCollection 2021.
Although scoring systems are widely used to predict outcomes in postcardiac arrest cardiogenic shock (CS) after out-of-hospital cardiac arrest (OHCA) complicating acute myocardial infarction (AMI), data concerning the accuracy of these scores to predict mortality of patients treated with Impella in this setting are lacking. Thus, we aimed to evaluate as well as to compare the prognostic accuracy of acute physiology and chronic health II (APACHE II), simplified acute physiology score II (SAPS II), sepsis-related organ failure assessment (SOFA), the intra-aortic balloon pump (IABP), CardShock, the prediction of cardiogenic shock outcome for AMI patients salvaged by VA-ECMO (ENCOURAGE), and the survival after venoarterial extracorporeal membrane oxygenation (SAVE) score in patients with OHCA refractory CS due to an AMI treated with Impella 2.5 or CP.
Retrospective study of 65 consecutive Impella 2.5 and 32 CP patients treated in our cardiac arrest center from September 2015 until June 2020.
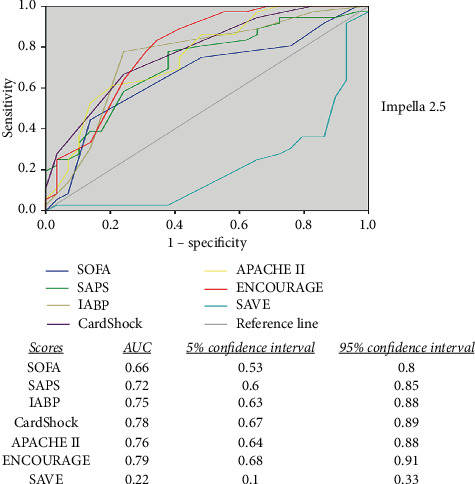
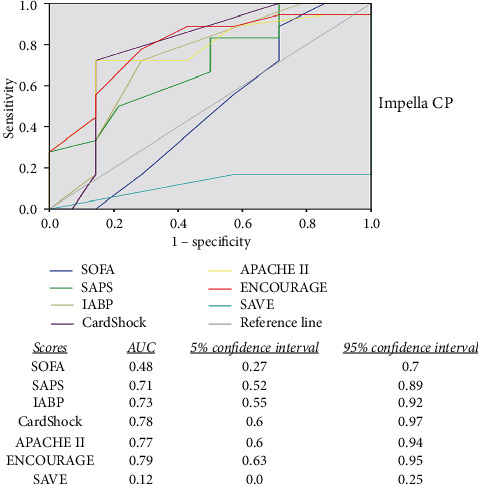
Overall survival to discharge was 44.3%. The expected mortality according to scores was SOFA 70%, SAPS II 90%, IABP shock 55%, CardShock 80%, APACHE II 85%, ENCOURAGE 50%, and SAVE score 70% in the 2.5 group; SOFA 70%, SAPS II 85%, IABP shock 55%, CardShock 80%, APACHE II 85%, ENCOURAGE 75%, and SAVE score 70% in the CP group. The ENCOURAGE score was the most effective predictive model of mortality outcome presenting a moderate area under the curve (AUC) of 0.79, followed by the CardShock, APACHE II, IABP, and SAPS score. These derived an AUC between 0.71 and 0.78. The SOFA and the SAVE scores failed to predict the outcome in this particular setting of refractory CS after OHCA due to an AMI.
The available intensive care and newly developed CS scores offered only a moderate prognostic accuracy for outcomes in OHCA patients with refractory CS due to an AMI treated with Impella. A new score is needed in order to guide the therapy in these patients.
尽管评分系统广泛用于预测院外心脏骤停(OHCA)并发急性心肌梗死(AMI)后心源性休克(CS)后心脏骤停后患者的预后,但关于这些评分系统预测在此情况下使用 Impella 治疗的患者死亡率的准确性的数据却很少。因此,我们旨在评估并比较急性生理学和慢性健康 II(APACHE II)、简化急性生理学评分 II(SAPS II)、脓毒症相关器官衰竭评估(SOFA)、主动脉内球囊泵(IABP)、CardShock、VA-ECMO 挽救的 AMI 患者心源性休克结局预测(ENCOURAGE)和静脉动脉体外膜肺氧合(SAVE)评分在因 AMI 导致的 OHCA 难治性 CS 患者中的预后准确性,这些患者接受 Impella 2.5 或 CP 治疗。
回顾性研究了 2015 年 9 月至 2020 年 6 月期间在我们心脏骤停中心接受 Impella 2.5 和 32 例 CP 治疗的 65 例连续患者。
总出院生存率为 44.3%。根据评分预测的死亡率为 SOFA 70%、SAPS II 90%、IABP 休克 55%、CardShock 80%、APACHE II 85%、ENCOURAGE 50%和 2.5 组中的 SAVE 评分 70%;SOFA 70%、SAPS II 85%、IABP 休克 55%、CardShock 80%、APACHE II 85%、ENCOURAGE 75%和 CP 组中的 SAVE 评分 70%。ENCOURAGE 评分是死亡率预测的最有效预测模型,曲线下面积(AUC)为 0.79,其次是 CardShock、APACHE II、IABP 和 SAPS 评分。这些评分的 AUC 在 0.71 到 0.78 之间。SOFA 和 SAVE 评分未能预测 AMI 后 OHCA 难治性 CS 患者的结局。
现有的重症监护评分和新开发的 CS 评分仅对因 AMI 导致的 OHCA 难治性 CS 患者的预后提供了中等的准确性,需要一种新的评分来指导这些患者的治疗。