Ranard Lauren S, Guber Kenneth, Fried Justin, Takeda Koji, Kaku Yuji, Karmpaliotis Dimitrios, Sayer Gabriel, Rabbani Leroy, Burkhoff Daniel, Uriel Nir, Kirtane Ajay J, Masoumi Amirali
Department of Cardiology, Columbia University Irving Medical Center, New York, New York, USA.
Department of Medicine, Columbia University Irving Medical Center, New York, New York, USA.
Struct Heart. 2022 Oct 31;6(6):100116. doi: 10.1016/j.shj.2022.100116. eCollection 2022 Nov.
There are numerous risk-prediction models applied to acute myocardial infarction-related cardiogenic shock (AMI-CS) patients to determine a more accurate prognosis and to assist in patient triage. There is wide heterogeneity among the risk models including the nature of predictors evaluated and their specific outcome measures. The aim of this analysis was to evaluate the performance of 20 risk-prediction models in AMI-CS patients.
Patients included in our analysis were admitted to a tertiary care cardiac intensive care unit with AMI-CS. Twenty risk-prediction models were computed utilizing vitals assessments, laboratory investigations, hemodynamic markers, and vasopressor, inotropic and mechanical circulatory support available from within the first 24 hours of presentation. Receiver operating characteristic curves were used to assess the prediction of 30-day mortality. Calibration was assessed with a Hosmer-Lemeshow test.
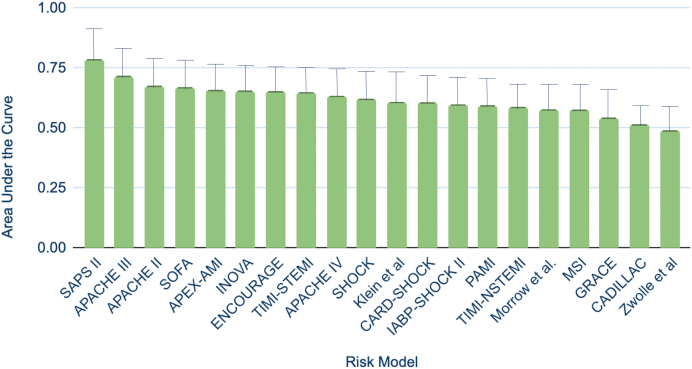
Seventy patients (median age 63 years, 67% male) were admitted between 2017 and 2021. The models' area under the curve (AUC) ranged from 0.49 to 0.79, with the Simplified Acute Physiology Score II score having the most optimal discrimination of 30-day mortality (AUC: 0.79, 95% confidence interval [CI]: 0.67-0.90), followed by the Acute Physiology and Chronic Health Evaluation-III score (AUC: 0.72, 95% CI: 0.59-0.84) and the Acute Physiology and Chronic Health Evaluation-II score (AUC: 0.67, 95% CI: 0.55-0.80). All 20 risk scores demonstrated adequate calibration ( > 0.05 for all).
Among the models tested in a data set of patients admitted with AMI-CS, the Simplified Acute Physiology Score II risk score model demonstrated the highest prognostic accuracy. Further investigations are required to improve the discriminative capabilities of these models or to establish new, more streamlined and accurate methods for mortality prognostication in AMI-CS.
有许多风险预测模型应用于急性心肌梗死相关的心源性休克(AMI-CS)患者,以确定更准确的预后并协助患者分诊。风险模型之间存在很大的异质性,包括评估的预测因素的性质及其特定的结局指标。本分析的目的是评估20种风险预测模型在AMI-CS患者中的性能。
纳入我们分析的患者为入住三级心脏重症监护病房的AMI-CS患者。利用生命体征评估、实验室检查、血流动力学指标以及入院后24小时内可用的血管升压药、正性肌力药和机械循环支持计算20种风险预测模型。采用受试者工作特征曲线评估30天死亡率的预测情况。用Hosmer-Lemeshow检验评估校准情况。
2017年至2021年间收治了70例患者(中位年龄63岁,67%为男性)。模型的曲线下面积(AUC)范围为0.49至0.79,简化急性生理学评分II对30天死亡率的区分能力最佳(AUC:0.79,95%置信区间[CI]:0.67-0.90),其次是急性生理学与慢性健康状况评估III评分(AUC:0.72,95%CI:0.59-0.84)和急性生理学与慢性健康状况评估II评分(AUC:0.67,95%CI:0.55-0.80)。所有20个风险评分均显示校准良好(所有P>0.05)。
在AMI-CS入院患者数据集中测试的模型中,简化急性生理学评分II风险评分模型显示出最高的预后准确性。需要进一步研究以提高这些模型的区分能力,或建立新的、更简化且准确的AMI-CS死亡率预后方法。