University of Gothenburg, Institute of Medicine, Department of Molecular and Clinical Medicine, Gothenburg, Sweden.
Centre for Clinical Research Dalarna, Uppsala University, S-79182 Falun, Sweden.
Eur Heart J. 2021 Mar 14;42(11):1094-1106. doi: 10.1093/eurheartj/ehaa1067.
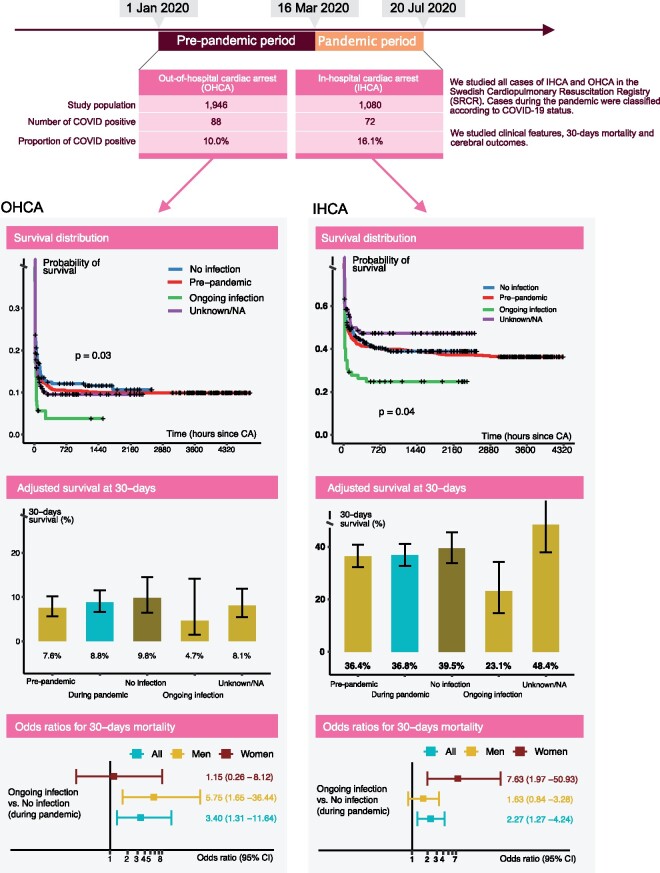
To study the characteristics and outcome among cardiac arrest cases with COVID-19 and differences between the pre-pandemic and the pandemic period in out-of-hospital cardiac arrest (OHCA) and in-hospital cardiac arrest (IHCA).
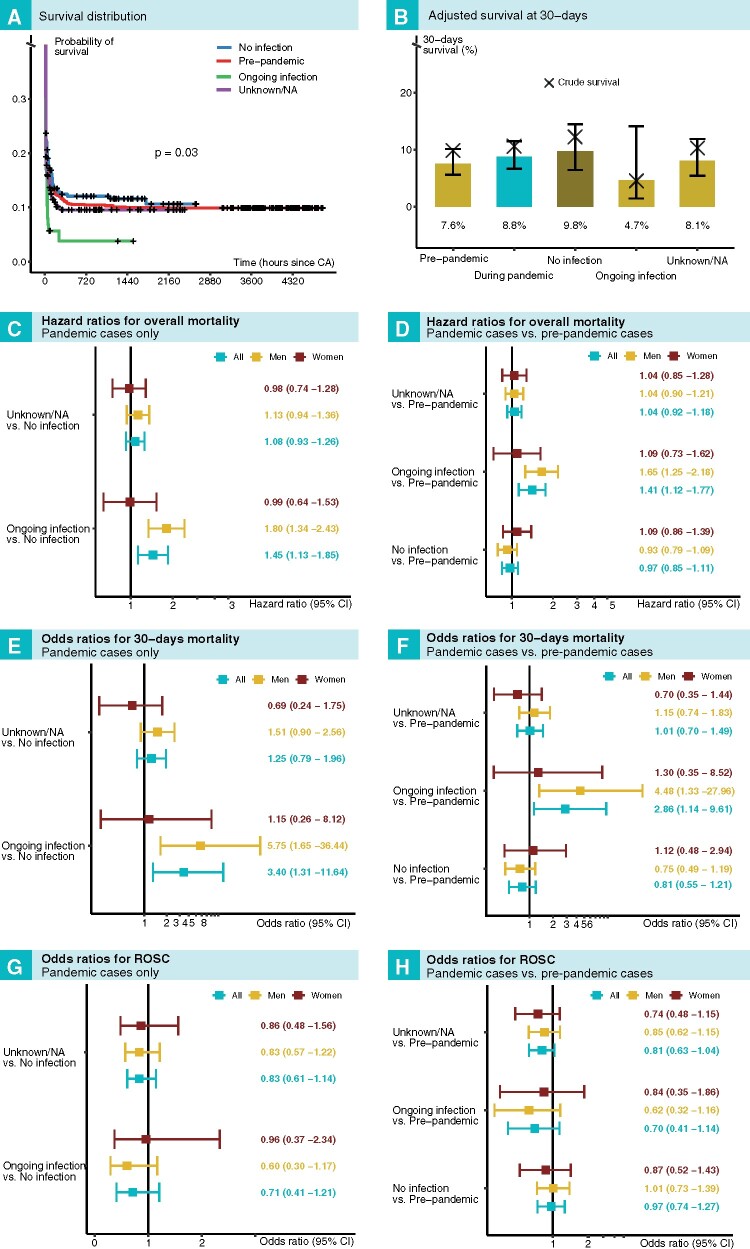
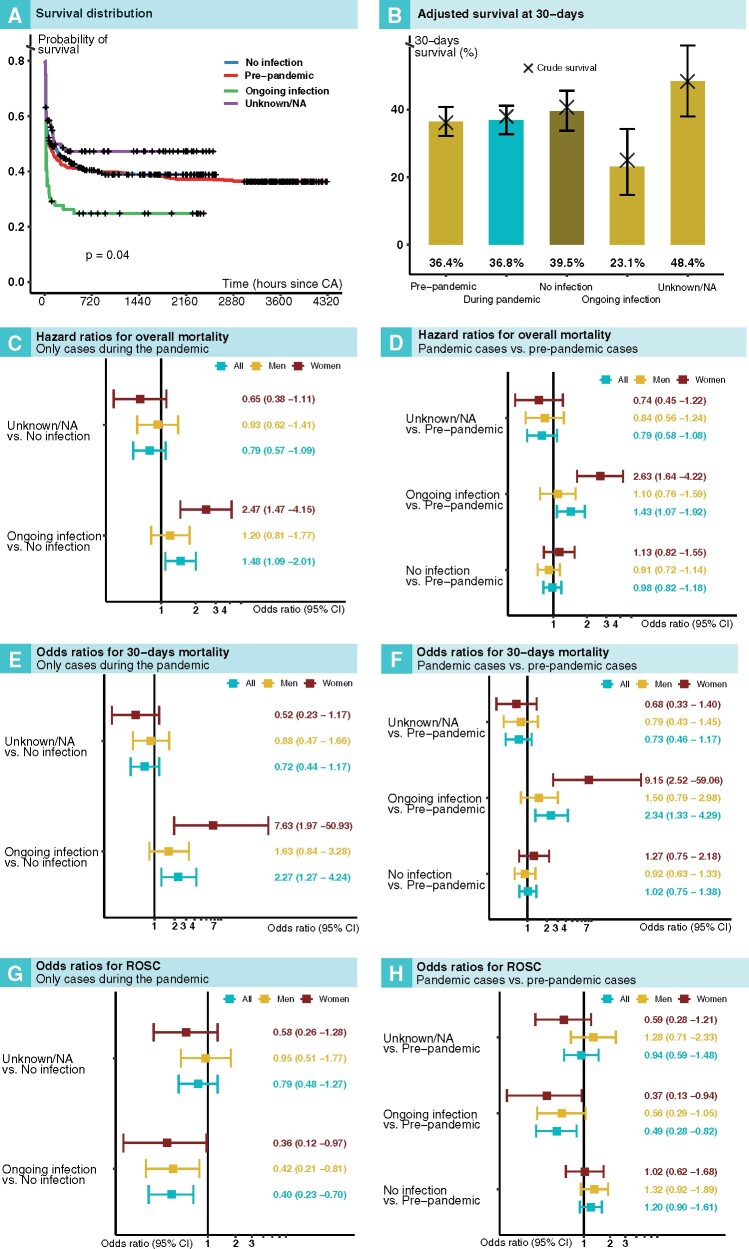
We included all patients reported to the Swedish Registry for Cardiopulmonary Resuscitation from 1 January to 20 July 2020. We defined 16 March 2020 as the start of the pandemic. We assessed overall and 30-day mortality using Cox regression and logistic regression, respectively. We studied 1946 cases of OHCA and 1080 cases of IHCA during the entire period. During the pandemic, 88 (10.0%) of OHCAs and 72 (16.1%) of IHCAs had ongoing COVID-19. With regards to OHCA during the pandemic, the odds ratio for 30-day mortality in COVID-19-positive cases, compared with COVID-19-negative cases, was 3.40 [95% confidence interval (CI) 1.31-11.64]; the corresponding hazard ratio was 1.45 (95% CI 1.13-1.85). Adjusted 30-day survival was 4.7% for patients with COVID-19, 9.8% for patients without COVID-19, and 7.6% in the pre-pandemic period. With regards to IHCA during the pandemic, the odds ratio for COVID-19-positive cases, compared with COVID-19-negative cases, was 2.27 (95% CI 1.27-4.24); the corresponding hazard ratio was 1.48 (95% CI 1.09-2.01). Adjusted 30-day survival was 23.1% in COVID-19-positive cases, 39.5% in patients without COVID-19, and 36.4% in the pre-pandemic period.
During the pandemic phase, COVID-19 was involved in at least 10% of all OHCAs and 16% of IHCAs, and, among COVID-19 cases, 30-day mortality was increased 3.4-fold in OHCA and 2.3-fold in IHCA.
研究 COVID-19 相关心搏骤停病例的特征和结局,并比较大流行前和大流行期间院外心搏骤停(OHCA)和院内心搏骤停(IHCA)之间的差异。
我们纳入了 2020 年 1 月 1 日至 7 月 20 日向瑞典心肺复苏登记处报告的所有患者。我们将 2020 年 3 月 16 日定义为大流行开始。我们分别使用 Cox 回归和逻辑回归评估总体和 30 天死亡率。我们研究了整个时期的 1946 例 OHCA 和 1080 例 IHCA。在大流行期间,88 例(10.0%)OHCA 和 72 例(16.1%)IHCA 持续存在 COVID-19。对于大流行期间的 OHCA,与 COVID-19 阴性病例相比,COVID-19 阳性病例 30 天死亡率的优势比为 3.40 [95%置信区间(CI)1.31-11.64];相应的风险比为 1.45(95%CI 1.13-1.85)。COVID-19 患者调整后的 30 天生存率为 4.7%,无 COVID-19 患者为 9.8%,大流行前为 7.6%。对于大流行期间的 IHCA,与 COVID-19 阴性病例相比,COVID-19 阳性病例的优势比为 2.27(95%CI 1.27-4.24);相应的风险比为 1.48(95%CI 1.09-2.01)。COVID-19 阳性病例调整后的 30 天生存率为 23.1%,无 COVID-19 患者为 39.5%,大流行前为 36.4%。
在大流行期间,COVID-19 至少占所有 OHCA 和 16%IHCA 的 10%,并且在 COVID-19 病例中,OHCA 中的 30 天死亡率增加了 3.4 倍,IHCA 中增加了 2.3 倍。