Department of Primary Care and Mental Health, Institute of Population Health Sciences, University of Liverpool, Liverpool, UK.
School of Psychology, Faculty of Health, Liverpool John Moores University, Liverpool, UK.
Acta Obstet Gynecol Scand. 2021 Jul;100(7):1288-1296. doi: 10.1111/aogs.14063. Epub 2021 Feb 5.
Despite widespread belief that anxiety causes longer labor, evidence of association is inconsistent. Data gathered as part of a prospective epidemiological longitudinal study were used to investigate associations between antenatal anxiety and pregnancy-specific stress, and labor progression was assessed by duration and use of augmentation.
Pregnant primiparous women completed measures for anxiety and pregnancy-specific stress at 20 weeks' gestation (n = 1145). Birth outcome data were extracted from medical records. Regression analyses and a path analysis assessed associations between antenatal anxiety and pregnancy-specific stress, and indices of labor progression (labor duration and augmentation).
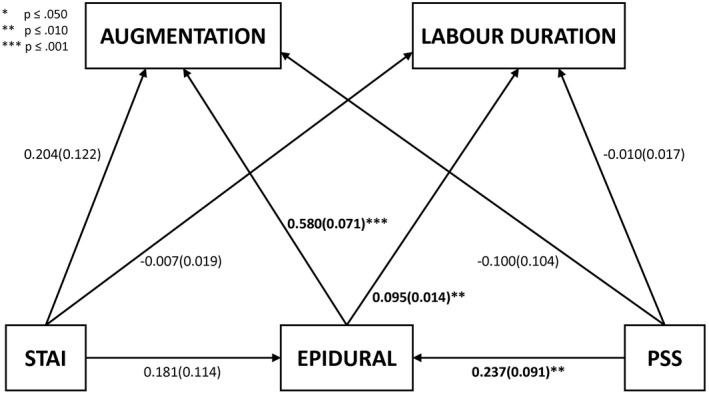
Anxiety/pregnancy-specific stress were not directly associated with duration of stage 1 labor (HIGH/LOW anxiety: mean difference = 13.94 minutes, SD = 20.66, 95% CI -26.60 to 54.49, P < .50)/(HIGH/LOW pregnancy-specific stress: mean difference = 12.05 minutes, SD = 16.09, 95% CI -19.52 to 43.63, P < .45). However, anxiety/pregnancy-specific stress were associated with epidural use (HIGH/LOW anxiety: 39% vs 31%, P < .042; HIGH/LOW pregnancy-specific stress: 38% vs 29%, P < .001), which was itself associated with longer labor (mean difference: 158.79 minutes, SD = 16.76, 95% CI 125.89-191.68, P < .001). Anxiety and pregnancy-specific stress were associated with increased likelihood of augmentation but these associations were nonsignificant after accounting for epidural, which was itself highly associated with augmentation. However, path analysis indicated an indirect effect linking pregnancy-specific stress, but not general anxiety, to labor duration and augmentation: elevated pregnancy-specific stress led to greater use of epidural, which was linked to both increased rates of augmentation, and increased labor duration.
Contrary to general belief, general anxiety and specific pregnancy stress were not directly linked to longer duration of stage one labor. However specific pregnancy stress was associated with epidural use, which in turn was significantly associated with risk of augmentation, and longer stage one labor. Identification of pregnancy-specific stress could help to identify women for whom psychological interventions could improve birth experience.
尽管普遍认为焦虑会导致分娩时间延长,但关联的证据并不一致。本研究使用前瞻性流行病学纵向研究中收集的数据,调查产前焦虑与妊娠特异性压力之间的关联,并通过持续时间和催产素使用评估产程进展。
1145 名初产妇在 20 周妊娠时完成焦虑和妊娠特异性压力的测量。从医疗记录中提取分娩结局数据。回归分析和路径分析评估了产前焦虑和妊娠特异性压力与产程进展(第一产程持续时间和催产素使用)的指标之间的关联。
焦虑/妊娠特异性压力与第一产程持续时间无直接关联(高/低焦虑:平均差异 13.94 分钟,SD 20.66,95%CI-26.60 至 54.49,P<0.50)/(高/低妊娠特异性压力:平均差异 12.05 分钟,SD 16.09,95%CI-19.52 至 43.63,P<0.45)。然而,焦虑/妊娠特异性压力与硬膜外使用相关(高/低焦虑:39%比 31%,P<0.042;高/低妊娠特异性压力:38%比 29%,P<0.001),而硬膜外使用本身与产程延长相关(平均差异:158.79 分钟,SD 16.76,95%CI 125.89 至 191.68,P<0.001)。焦虑和妊娠特异性压力与催产素使用率增加相关,但在考虑到硬膜外使用后,这些关联无统计学意义,而硬膜外使用本身与催产素使用率高度相关。然而,路径分析表明,特定于妊娠的压力与产程时间和催产素使用之间存在间接关联:妊娠特异性压力增加导致硬膜外使用率增加,这与催产素使用率增加和第一产程时间延长有关。
与普遍观点相反,一般焦虑和特定于妊娠的压力与第一产程持续时间的延长没有直接关系。然而,特定于妊娠的压力与硬膜外使用有关,而硬膜外使用又与催产素使用率增加和第一产程时间延长显著相关。识别妊娠特异性压力可以帮助识别那些可能通过心理干预改善分娩体验的女性。