Renal, Electrolyte-Hypertension Division, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania.
Center for Clinical Epidemiology and Biostatistics, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, Pennsylvania.
J Am Soc Nephrol. 2021 Mar;32(3):663-675. doi: 10.1681/ASN.2020040394. Epub 2021 Feb 5.
Adherence to healthy behaviors reduces risks of cardiovascular disease and death in the general population. However, among people with kidney disease, a group at higher risk for cardiovascular disease, such benefits have not been established.
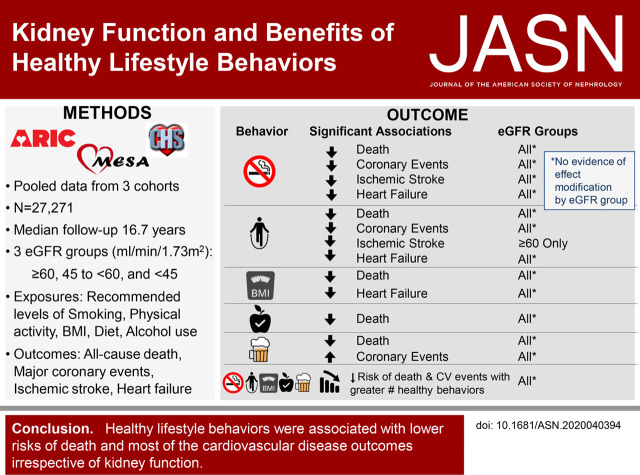
We pooled data from three cohort studies with a total of 27,271 participants. Kidney function was categorized on the basis of eGFR (≥60, 45 to <60, and <45 ml/min per 1.73 m). We used proportional hazard frailty models to estimate associations between healthy behaviors (not smoking, at recommended body mass index [BMI], physical activity, healthy diet, and moderate to no alcohol intake) and outcomes (all-cause death, major coronary events, ischemic stroke, and heart failure events).
All recommended lifestyle behaviors were significantly associated with lower risks of death, regardless of eGFR. Not smoking (versus current) and any moderate to vigorous physical activity (versus none) was significantly associated with reduced risks of major coronary and heart failure events, regardless of eGFR. Any (versus no) moderate or vigorous physical activity significantly associated with decreased risk of ischemic stroke events only among those with eGFR ≥60. Moderate to no daily alcohol intake (versus excessive) was significantly associated with an increased risk of major coronary events, regardless of eGFR. For heart failure events, a BMI of 18.5 to 30 associated with decreased risk, regardless of eGFR. Across all eGFR categories, the magnitude of risk reduction for death and all cardiovascular outcomes increased with greater numbers of recommended lifestyle behaviors.
Recommended lifestyle behaviors are associated with lower risk of death and cardiovascular disease events among individuals with or without reduced kidney function, supporting lifestyle behaviors as potentially modifiable risk factors for people with kidney disease.
在普通人群中,坚持健康的行为可降低心血管疾病和死亡的风险。然而,在肾病患者(心血管疾病风险较高的人群)中,尚未确定这些益处。
我们汇总了三项队列研究的数据,共纳入 27271 名参与者。根据 eGFR(≥60、45 至<60 和<45 ml/min/1.73 m)将肾功能分类。我们使用比例风险脆弱性模型来估计健康行为(不吸烟、推荐的体重指数 [BMI]、体力活动、健康饮食和适量或不饮酒)与结局(全因死亡、主要冠状动脉事件、缺血性卒中和心力衰竭事件)之间的关联。
无论 eGFR 如何,所有推荐的生活方式行为均与较低的死亡风险显著相关。不吸烟(与当前吸烟相比)和任何中等强度或剧烈体力活动(与无体力活动相比)与降低主要冠状动脉和心力衰竭事件的风险显著相关,无论 eGFR 如何。任何(与无)中等强度或剧烈体力活动仅与 eGFR≥60 的人群发生缺血性卒事件的风险降低显著相关。适量或不饮酒(与过量饮酒相比)与全因死亡风险增加显著相关,无论 eGFR 如何。对于心力衰竭事件,BMI 为 18.5 至 30 与降低风险相关,无论 eGFR 如何。在所有 eGFR 类别中,随着推荐的生活方式行为数量的增加,死亡和所有心血管结局的风险降低幅度也随之增加。
在肾功能降低或不降低的个体中,推荐的生活方式行为与死亡和心血管疾病事件的风险降低相关,这支持了将生活方式行为作为肾病患者潜在的可改变风险因素。