Département de Médecine Interne, Hôpital Bichat, Assistance Publique Hôpitaux de Paris, Université de Paris, France.
Département d'Hémostase, Hôpital Bichat, Assistance Publique Hôpitaux de Paris, Université de Paris, France.
Mayo Clin Proc. 2021 Feb;96(2):295-303. doi: 10.1016/j.mayocp.2020.11.018. Epub 2020 Nov 27.
To evaluate the clinical course of and risk factors for arterial thrombotic events in adult inpatients with coronavirus disease 2019 (COVID-19).
All consecutive adult patients admitted for COVID-19 infection in a referral center in France and discharged from the hospital between April 1 and April 30, 2020, were included. All arterial thrombotic events that occurred through discharge were considered for analysis. Epidemiologic, demographic, clinical, laboratory, treatment, and outcome data were extracted from electronic medical records with use of a standardized data collection form.
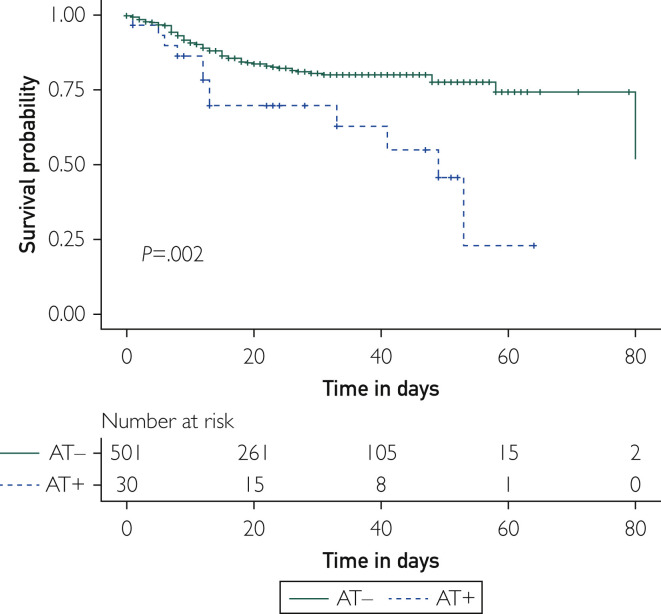
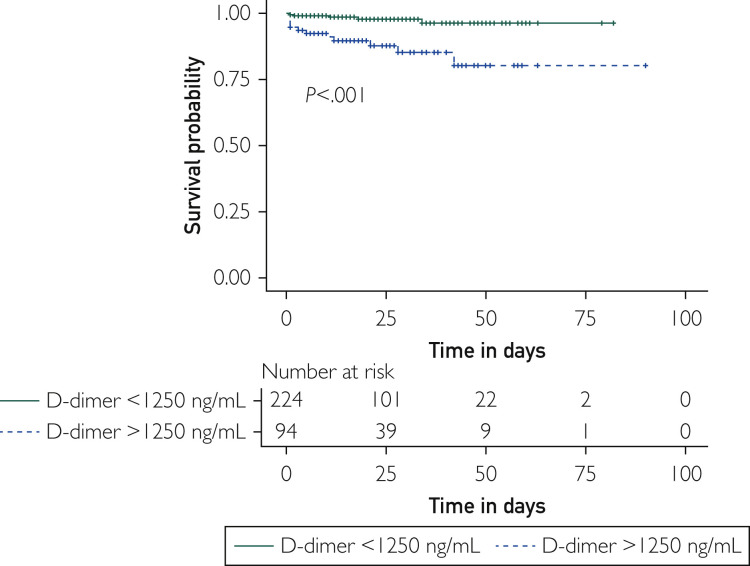
Overall, 531 COVID-19+ patients were analyzed. Among them, 30 (5.6%) experienced arterial thrombotic events. Arterial thrombotic events in the setting of COVID-19 infection happened at a median of 11 (5-20) days after the first symptoms of infection; occurred in high-risk patients according to traditional cardiovascular risk factors; had an atypical pattern, such as thrombosis of the aorta, upper limb, or renal arteries or cerebral microvasculopathy in 7 (23.3%) cases; and were associated with an in-hospital mortality rate of 40%. Arterial thrombotic events increased the risk of death by 3-fold in COVID-19+ patients (hazard ratio, 2.96; 95% CI, 1.4 to 4.7; P=.002). A subdistribution survival hazard model showed that a concentration of D-dimer above 1250 ng/mL increased the risk of arterial thrombotic events in COVID-19+ patients by more than 7 (subdistribution hazard ratio, 7.68; 95% CI, 2.9 to 20.6; P<.001).
A dramatically high rate of in-hospital death was observed in patients who suffered arterial thrombotic events in the setting of COVID-19 infection. A D-dimer level above 1250 ng/mL at entry may identify COVID-19+ patients at risk for arterial thrombotic events.
评估成人 2019 冠状病毒病(COVID-19)住院患者动脉血栓事件的临床过程和相关危险因素。
纳入 2020 年 4 月 1 日至 4 月 30 日期间在法国一家转诊中心因 COVID-19 感染而住院并出院的所有连续成年患者。分析所有出院时发生的动脉血栓事件。从电子病历中提取流行病学、人口统计学、临床、实验室、治疗和结局数据,并使用标准化数据采集表进行分析。
共分析了 531 例 COVID-19+患者。其中 30 例(5.6%)发生动脉血栓事件。COVID-19 感染背景下的动脉血栓事件发生在感染首发症状后 11(5-20)天中位数;发生在传统心血管危险因素高危患者中;具有非典型模式,如主动脉、上肢或肾动脉血栓形成或 7 例(23.3%)患者的脑微血管病;与院内死亡率 40%相关。动脉血栓事件使 COVID-19+患者的死亡风险增加 3 倍(危险比,2.96;95%CI,1.4 至 4.7;P=.002)。亚分布生存风险模型显示,D-二聚体浓度高于 1250ng/mL 使 COVID-19+患者发生动脉血栓事件的风险增加超过 7 倍(亚分布危险比,7.68;95%CI,2.9 至 20.6;P<.001)。
在 COVID-19 感染背景下发生动脉血栓事件的患者观察到极高的院内死亡率。入院时 D-二聚体水平高于 1250ng/mL 可能识别出有发生动脉血栓事件风险的 COVID-19+患者。