Epidemic Intelligence Service, Centers for Disease Control and Prevention, Atlanta, GA, USA; CDC COVID-19 Emergency Response, Atlanta, GA, USA.
Epidemic Intelligence Service, Centers for Disease Control and Prevention, Atlanta, GA, USA; CDC COVID-19 Emergency Response, Atlanta, GA, USA.
J Am Med Dir Assoc. 2021 Mar;22(3):498-503. doi: 10.1016/j.jamda.2021.01.070. Epub 2021 Jan 28.
Effective halting of outbreaks in skilled nursing facilities (SNFs) depends on the earliest recognition of cases. We assessed confirmed COVID-19 cases at an SNF impacted by COVID-19 in the United States to identify early indications of COVID-19 infection.
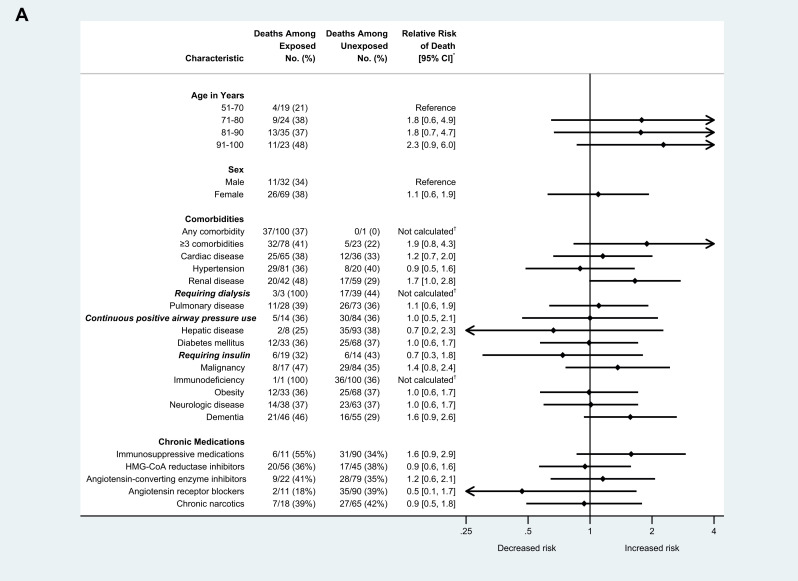
We performed retrospective reviews of electronic health records for residents with laboratory-confirmed SARS-CoV-2 during February 28-March 16, 2020. Records were abstracted for comorbidities, signs and symptoms, and illness outcomes during the 2 weeks before and after the date of positive specimen collection. Relative risks (RRs) of hospitalization and death were calculated.
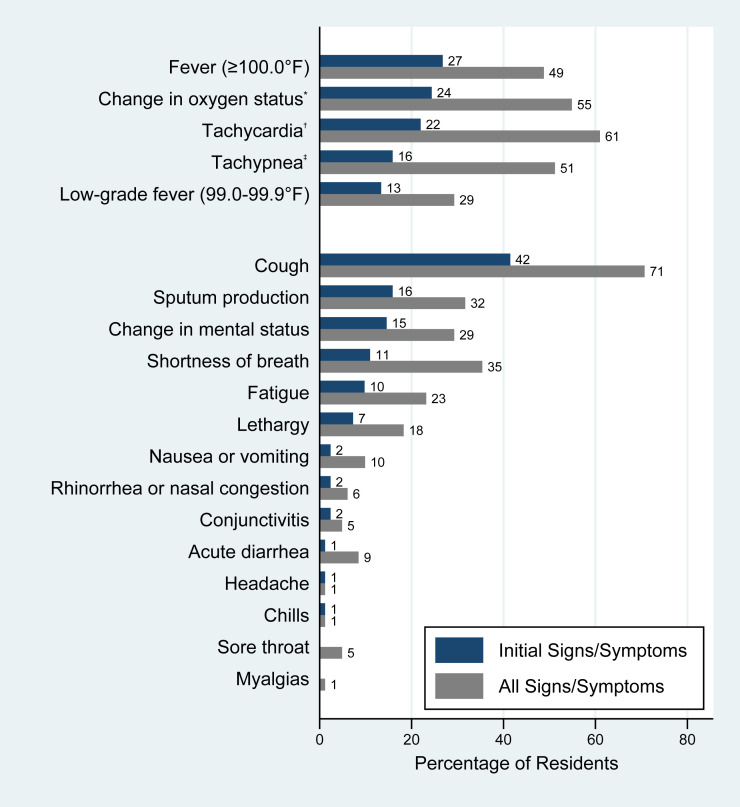
Of the 118 residents tested among approximately 130 residents from Facility A during February 28-March 16, 2020, 101 (86%) were found to test positive for SARS-CoV-2. At initial presentation, about two-thirds of SARS-CoV-2-positive residents had an abnormal vital sign or change in oxygen status. Most (90.2%) symptomatic residents had elevated temperature, change in mental status, lethargy, change in oxygen status, or cough; 9 (11.0%) did not have fever, cough, or shortness of breath during their clinical course. Those with change in oxygen status had an increased relative risk (RR) of 30-day mortality [51.1% vs 29.7%, RR 1.7, 95% confidence interval (CI) 1.0-3.0]. RR of hospitalization was higher for residents with underlying hepatic disease (1.6, 95% CI 1.1-2.2) or obesity (1.5, 95% CI 1.1-2.1); RR of death was not statistically significant.
Our findings reinforce the critical role that monitoring of signs and symptoms can have in identifying COVID-19 cases early. SNFs should ensure they have a systematic approach for responding to abnormal vital signs and oxygen saturation and consider ensuring common signs and symptoms identified in Facility A are among those they monitor.
在熟练护理机构 (SNF) 中有效阻止疫情爆发取决于对病例的最早识别。我们评估了受新冠疫情影响的 SNF 中确诊的 COVID-19 病例,以确定 COVID-19 感染的早期迹象。
我们对 2020 年 2 月 28 日至 3 月 16 日期间实验室确诊为 SARS-CoV-2 的居民的电子健康记录进行了回顾性分析。记录了在阳性标本采集日期前后两周内的合并症、体征和症状以及疾病结局。计算了住院和死亡的相对风险 (RR)。
在 2020 年 2 月 28 日至 3 月 16 日期间,对设施 A 的约 130 名居民进行了 118 次检测,其中 101 名(86%)检测结果为 SARS-CoV-2 阳性。在初次就诊时,大约三分之二的 SARS-CoV-2 阳性居民有异常生命体征或血氧状态变化。大多数(90.2%)有症状的居民出现体温升高、精神状态改变、乏力、血氧状态改变或咳嗽;9 名(11.0%)在其临床过程中没有发热、咳嗽或呼吸急促。有血氧状态改变的患者 30 天死亡率的相对风险增加(51.1% vs 29.7%,RR 1.7,95%置信区间[CI] 1.0-3.0)。患有基础性肝病(1.6,95%CI 1.1-2.2)或肥胖症(1.5,95%CI 1.1-2.1)的居民住院的 RR 较高;死亡的 RR 无统计学意义。
我们的研究结果强化了监测体征和症状在早期识别 COVID-19 病例方面的重要作用。护理机构应确保他们有系统的方法来应对异常生命体征和血氧饱和度,并考虑确保设施 A 中确定的常见体征和症状在他们监测的范围内。