Department of Nuclear Medicine. Inselspital, Bern University Hospital, University of Bern, Street: Freiburgstr. 18, CH-3010, Bern, Switzerland.
Institute of Medical Biometry and Informatics, University of Heidelberg, Im Neuenheimer Feld 130.3, 69120, Heidelberg, Germany.
Eur J Nucl Med Mol Imaging. 2021 Aug;48(9):2978-2989. doi: 10.1007/s00259-021-05210-9. Epub 2021 Feb 6.
Many radiotracers are currently available for the detection of recurrent prostate cancer (rPC), yet many have not been compared head-to-head in comparative imaging studies. There is therefore an unmet need for evidence synthesis to guide evidence-based decisions in the selection of radiotracers. The objective of this study was therefore to assess the detection rate of various radiotracers for the rPC.
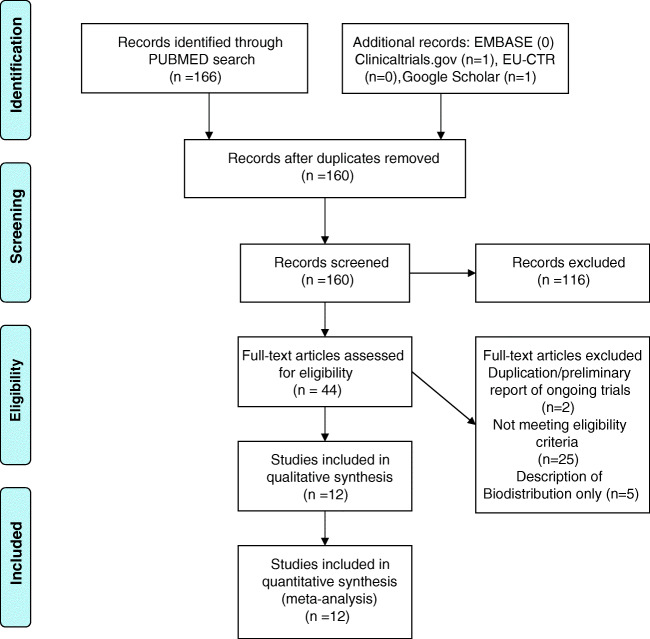
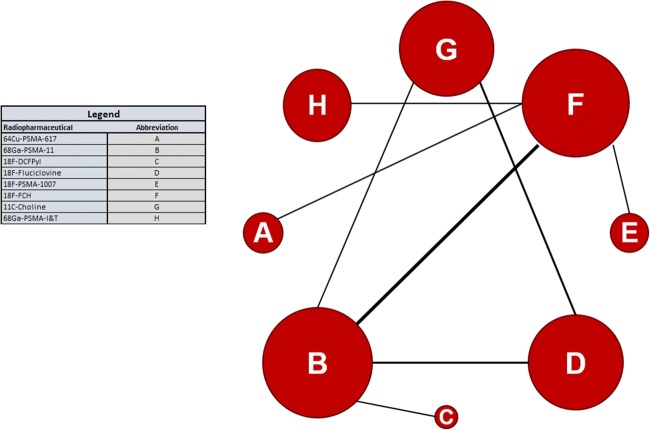
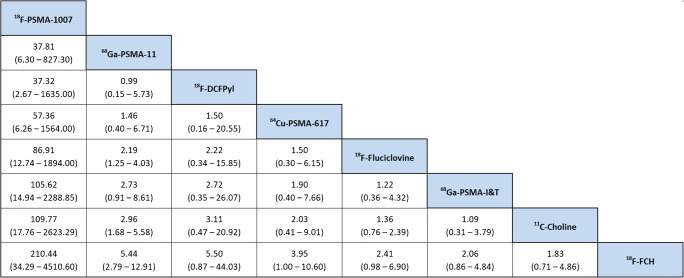
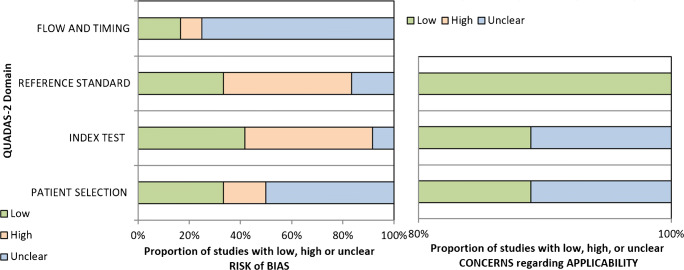
The PUBMED, EMBASE, and the EU and NIH trials databases were searched without date or language restriction for comparative imaging tracers for 13 radiotracers of principal interest. Key search terms included 18F-PSMA-1007, 18F-DCPFyl, 68Ga-PSMA-11, 18F-PSMA-11, 68Ga-PSMA-I&T, 68Ga-THP-PSMA, 64Cu-PSMA-617, 18F-JK-PSMA-7, 18F-Fluciclovine, 18F-FABC, 18F-Choline, 11C-Choline, and 68Ga-RM2. Studies reporting comparative imaging data in humans in rPC were selected. Single armed studies and matched pair analyses were excluded. Twelve studies with eight radiotracers were eligible for inclusion. Two independent reviewers screened all studies (using the PRISMA-NMA statement) for inclusion criteria, extracted data, and assessed risk of bias (using the QUADAS-2 tool). A network meta-analysis was performed using Markov-Chain Monte Carlo Bayesian analysis to obtain estimated detection rate odds ratios for each tracer combination.
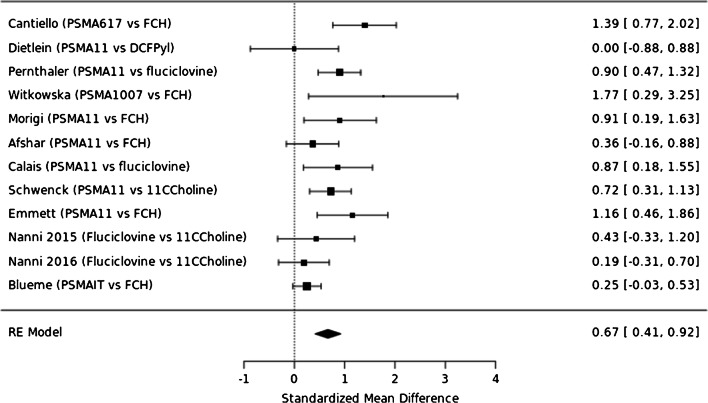
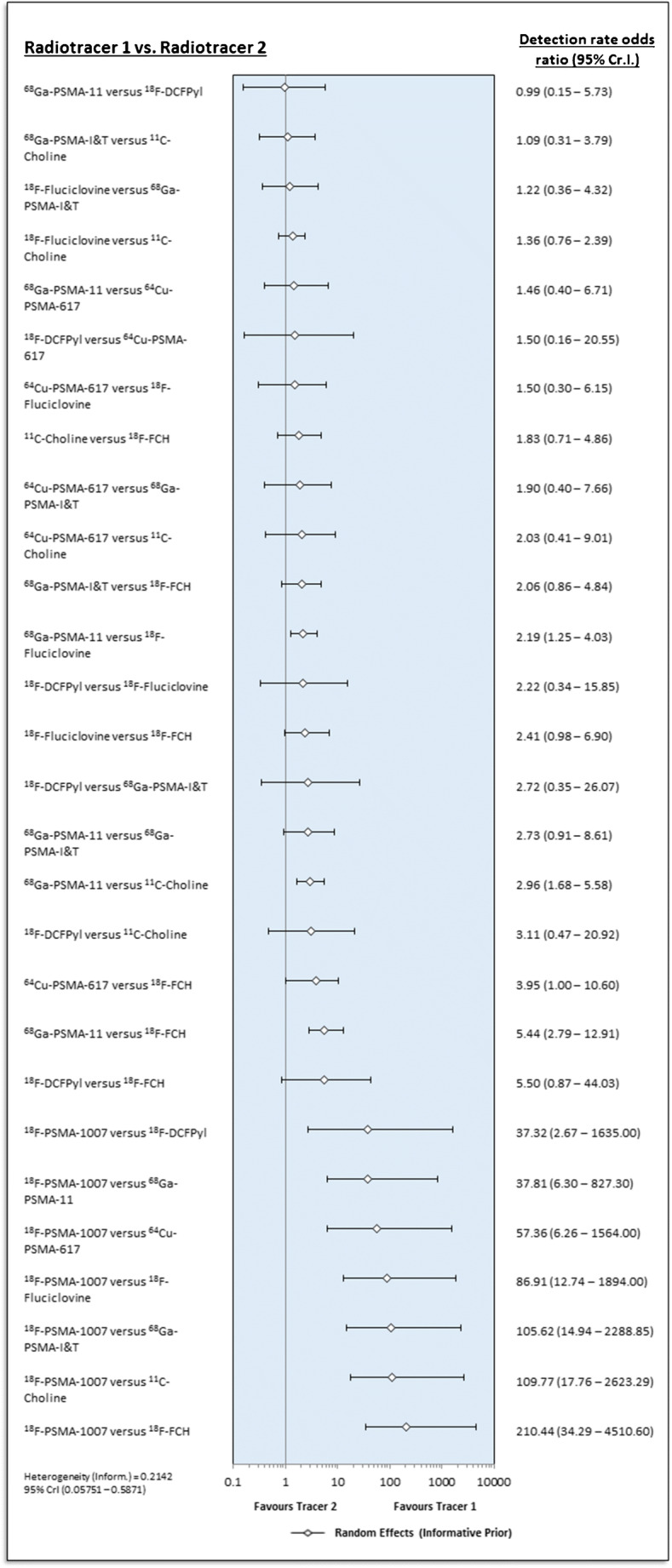
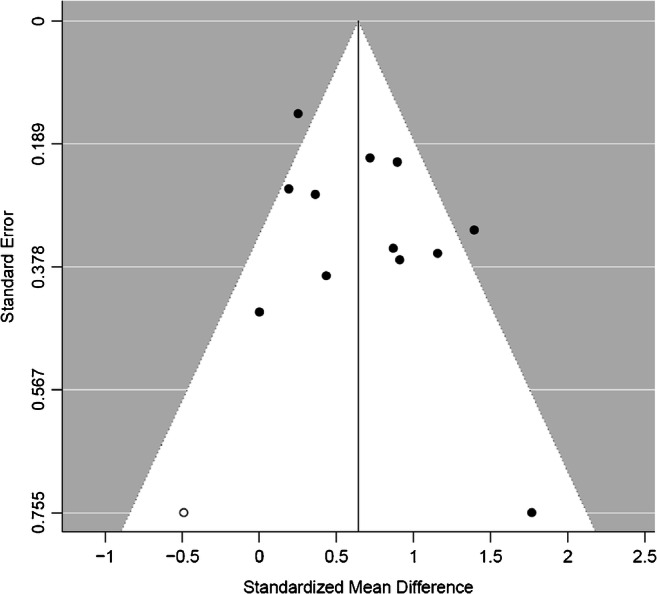
A majority of studies were judged to be at risk of publication bias. With the exception of 18F-PSMA-1007, little difference in terms of detection rate was revealed between the three most commonly used PSMA-radiotracers (Ga-PSMA-11, F-PSMA-1007, F-DCFPyl), which in turn showed clear superiority to choline and fluciclovine using the derived network.
Differences in patient-level detection rates were observed between PSMA- and choline-radiotracers. However, there is currently insufficient evidence to favour one of the four routinely used PSMA-radioligands (PSMA-11, PSMA-1007, PSMA-I&T, and DCFPyl) over another owing to the limited evidence base and risk of publication bias revealed by our systematic review. A further limitation was lack of reporting on diagnostic accuracy, which might favour radiotracers with low specificity in an analysis restricted only to detection rate. The NMA derived can be used to inform the design of future clinical trials and highlight areas where current evidence is weak.
目前有许多放射性示踪剂可用于检测复发性前列腺癌(rPC),但在比较影像学研究中,许多示踪剂尚未进行头对头比较。因此,需要进行证据综合,以指导放射性示踪剂选择的循证决策。本研究的目的是评估各种放射性示踪剂检测 rPC 的检出率。
在没有日期或语言限制的情况下,检索 PUBMED、EMBASE 和欧盟及 NIH 试验数据库,以查找 13 种主要感兴趣的放射性示踪剂的比较影像学示踪剂。主要检索词包括 18F-PSMA-1007、18F-DCPFyl、68Ga-PSMA-11、18F-PSMA-11、68Ga-PSMA-I&T、68Ga-THP-PSMA、64Cu-PSMA-617、18F-JK-PSMA-7、18F-Fluciclovine、18F-FABC、18F-Choline、11C-Choline 和 68Ga-RM2。选择报告 rPC 中比较影像学数据的研究。排除单臂研究和配对分析。符合纳入标准的有 12 项研究,涉及 8 种放射性示踪剂。两名独立评审员(使用 PRISMA-NMA 声明)筛选所有研究以确定纳入标准、提取数据和评估偏倚风险(使用 QUADAS-2 工具)。使用马尔可夫链蒙特卡罗贝叶斯分析进行网络荟萃分析,以获得每个示踪剂组合的估计检出率优势比。
大多数研究被认为存在发表偏倚的风险。除 18F-PSMA-1007 外,三种最常用的 PSMA 放射性示踪剂(Ga-PSMA-11、F-PSMA-1007、F-DCFPyl)之间的检出率差异不大,而根据所得网络,这三种示踪剂明显优于胆碱和氟尿苷。
在 PSMA 和胆碱放射性示踪剂之间观察到患者水平检测率的差异。然而,由于系统评价中揭示的证据基础有限和发表偏倚风险,目前尚无足够的证据支持四种常规使用的 PSMA 放射性配体(PSMA-11、PSMA-1007、PSMA-I&T 和 DCFPyl)中的一种优于另一种。另一个限制是缺乏诊断准确性的报告,这可能有利于在仅基于检出率的分析中特异性较低的放射性示踪剂。所得到的 NMA 可用于为未来的临床试验提供信息,并突出当前证据薄弱的领域。