Department of Gastrointestinal Oncology, National Cancer Center Hospital East, Kashiwa, Chiba, Japan.
Department of Clinical Oncology, Aichi Cancer Center Hospital, Nagoya, Japan.
ESMO Open. 2020;5(1):e000624. doi: 10.1136/esmoopen-2019-000624. Epub 2020 Sep 30.
While the BRAF V600E mutation occurs in 5%-15% of metastatic colorectal cancer (mCRC), BRAF non-V600E mutations were recently reported to range from 1.6% to 5.1%. We have previously reported that BRAF non-V600E mutations could have a negative impact on efficacy outcomes as well as BRAF V600E mutation for antiepidermal growth factor receptor (EGFR) antibody treatment for pretreated patients with mCRC. Recently, simultaneous inhibitions of mitogen-activated protein kinase kinase (MEK), BRAF and EGFR exhibited relevant antitumour activities in patients with BRAF V600E mutant and also in BRAF non-V600E mutant but only in the preclinical model.
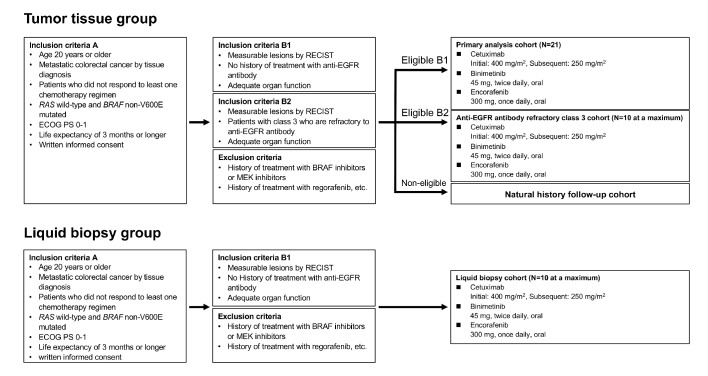
The BIG BANG (study is a multicentre, phase II study to assess the efficacy, safety and proof of concept of the combinations of binimetinib+encorafenib+cetuximab in patients with BRAF non-V600E mutated mCRC, identified by either tumour tissue (tumour tissue group) or blood samples (liquid biopsy group). Key eligibility criteria include Eastern Cooperative Oncology Group Performance Status of ≤1, mCRC with BRAF non-V600E mutant and RAS wild type, refractory or intolerant to at least one fluoropyrimidine-based regimen and no prior history of regorafenib, and no prior history of anti-EGFR antibody treatment (primary analysis cohort and liquid biopsy cohort) or refractory to prior anti-EGFR antibody treatment in patients with class 3 BRAF mutations (anti-EGFR antibody refractory class three cohort). Enrolled patients receive binimetinib (45 mg, two times per day), encorafenib (300 mg, once a day) and cetuximab (initially 400 mg/m and subsequently 250 mg/m, once per week). The primary endpoint is the confirmed objective response rate in the primary analysis cohort.
UMIN000031857 and 000031860.
虽然 BRAF V600E 突变发生在 5%-15%的转移性结直肠癌(mCRC)中,但最近报道 BRAF 非 V600E 突变的范围为 1.6%-5.1%。我们之前报道过,BRAF 非 V600E 突变可能对疗效产生负面影响,以及 BRAF V600E 突变对预处理的 mCRC 患者抗表皮生长因子受体(EGFR)抗体治疗的影响。最近,丝裂原活化蛋白激酶激酶(MEK)、BRAF 和 EGFR 的同时抑制在 BRAF V600E 突变和 BRAF 非 V600E 突变的患者中以及仅在临床前模型中显示出相关的抗肿瘤活性。
BIG BANG(研究是一项多中心、II 期研究,旨在评估 binimetinib+encorafenib+cetuximab 联合治疗 BRAF 非 V600E 突变 mCRC 患者的疗效、安全性和概念验证,通过肿瘤组织(肿瘤组织组)或血液样本(液体活检组)确定。主要入选标准包括东部合作肿瘤组(ECOG)表现状态≤1、BRAF 非 V600E 突变且 RAS 野生型的 mCRC、对至少一种氟嘧啶类方案难治或不耐受且无regorafenib 治疗史,以及无抗 EGFR 抗体治疗史(主要分析队列和液体活检队列)或对 3 类 BRAF 突变患者的抗 EGFR 抗体治疗难治(抗 EGFR 抗体难治 3 类队列)。入组患者接受 binimetinib(45 mg,每日两次)、encorafenib(300 mg,每日一次)和 cetuximab(初始 400 mg/m,随后 250 mg/m,每周一次)。主要终点是主要分析队列中确认的客观缓解率。
UMIN000031857 和 000031860。