Peng Gang, Tang Yishuo, Cowan Tina M, Zhao Hongyu, Scharfe Curt
Department of Genetics, Yale University School of Medicine, New Haven, CT, United States.
Department of Biostatistics, Yale University School of Public Health, New Haven, CT, United States.
Front Pediatr. 2021 Jan 20;8:623184. doi: 10.3389/fped.2020.623184. eCollection 2020.
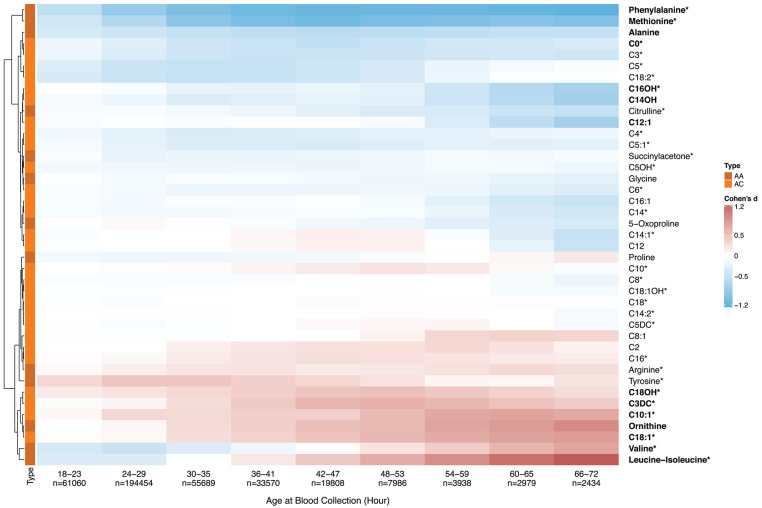
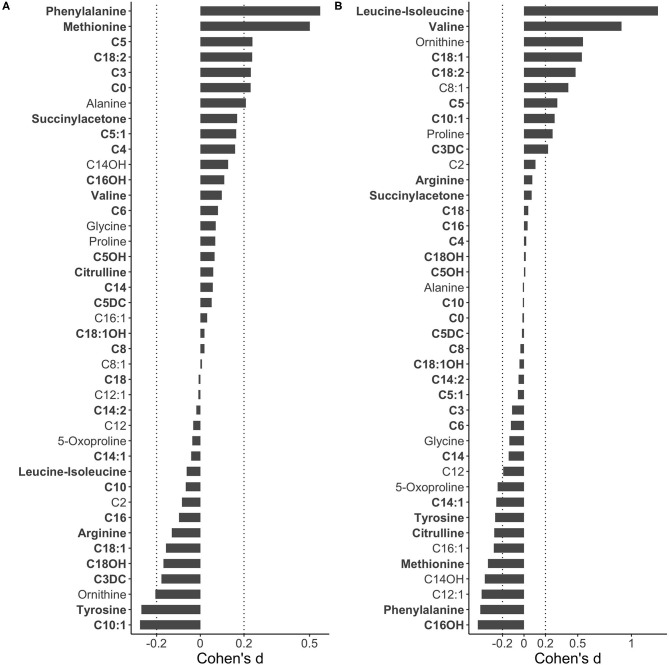
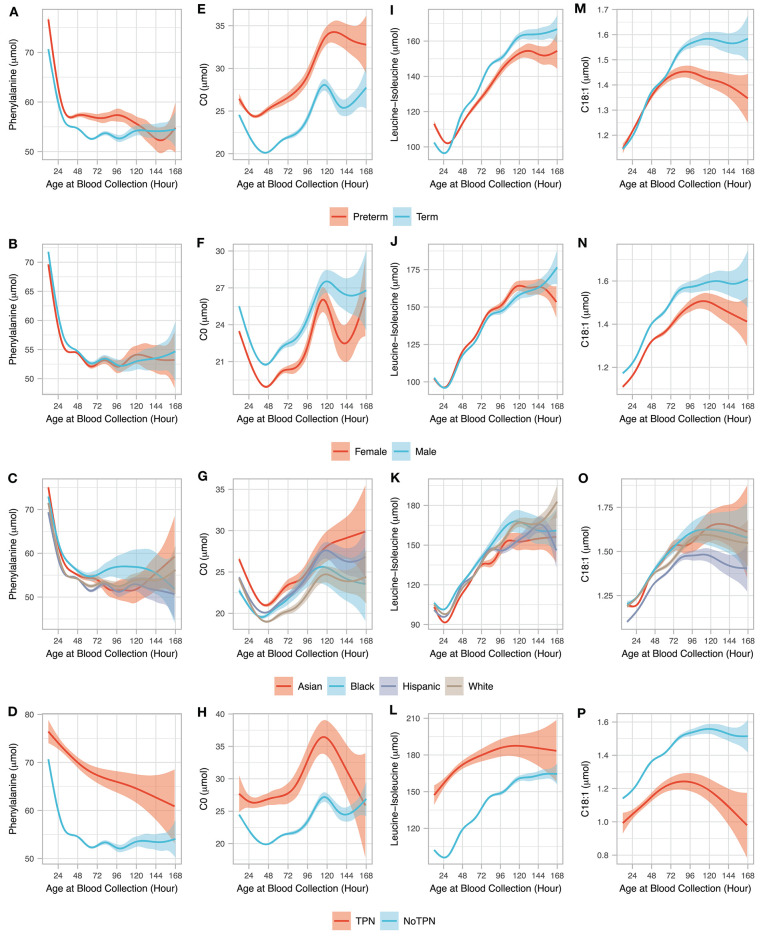
Blood collection for newborn genetic disease screening is preferably performed within 24-48 h after birth. We used population-level newborn screening (NBS) data to study early postnatal metabolic changes and whether timing of blood collection could impact screening performance. Newborns were grouped based on their reported age at blood collection (AaBC) into early (12-23 h), standard (24-48 h), and late (49-168 h) collection groups. Metabolic marker levels were compared between the groups using effect size analysis, which controlled for group size differences and influence from the clinical variables of birth weight and gestational age. Metabolite level differences identified between groups were correlated to NBS data from false-positive cases for inborn metabolic disorders including carnitine transport defect (CTD), isovaleric acidemia (IVA), methylmalonic acidemia (MMA), and phenylketonuria (PKU). Our results showed that 56% of the metabolites had AaBC-related differences, which included metabolites with either decreasing or increasing levels after birth. Compared to the standard group, the early-collection group had elevated marker levels for PKU (phenylalanine, Cohen's = 0.55), IVA (C5, Cohen's = 0.24), MMA (C3, Cohen's = 0.23), and CTD (C0, Cohen's = 0.23). These findings correlated with higher false-positive rates for PKU ( < 0.05), IVA ( < 0.05), and MMA ( < 0.001), and lower false-positive rate for CTD ( < 0.001) in the early-collection group. Blood collection before 24 h could affect screening performance for some metabolic disorders. We have developed web-based tools integrating AaBC and other variables for interpretive analysis of screening data.
新生儿遗传疾病筛查的采血最好在出生后24 - 48小时内进行。我们使用人群水平的新生儿筛查(NBS)数据来研究出生后早期的代谢变化以及采血时间是否会影响筛查性能。根据报告的采血年龄(AaBC)将新生儿分为早期(12 - 23小时)、标准(24 - 48小时)和晚期(49 - 168小时)采血组。使用效应量分析比较各组之间的代谢标志物水平,该分析控制了组大小差异以及出生体重和胎龄等临床变量的影响。在各组之间确定的代谢物水平差异与先天性代谢紊乱(包括肉碱转运缺陷(CTD)、异戊酸血症(IVA)、甲基丙二酸血症(MMA)和苯丙酮尿症(PKU))假阳性病例的NBS数据相关。我们的结果表明,56%的代谢物具有与AaBC相关的差异,其中包括出生后水平降低或升高的代谢物。与标准组相比,早期采血组中PKU(苯丙氨酸,科恩效应量 = 0.55)、IVA(C5,科恩效应量 = 0.24)、MMA(C3,科恩效应量 = 0.23)和CTD(C0,科恩效应量 = 0.23)的标志物水平升高。这些发现与早期采血组中PKU(<0.05)、IVA(<0.05)和MMA(<0.001)较高的假阳性率以及CTD(<0.001)较低的假阳性率相关。24小时前采血可能会影响某些代谢紊乱的筛查性能。我们开发了基于网络的工具,整合了AaBC和其他变量,用于筛查数据的解释性分析。