Pharmaceutical Outcomes and PolicyCollege of PharmacyUniversity of FloridaGainesvilleFLUSA.
Department of Epidemiology, College of Public Health and Health Professions and College of MedicineUniversity of FloridaGainesvilleFLUSA.
Hepatol Commun. 2020 Nov 17;5(2):203-216. doi: 10.1002/hep4.1634. eCollection 2021 Feb.
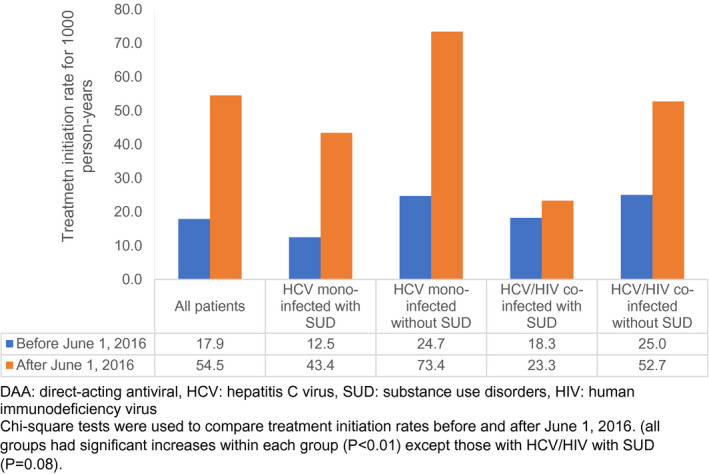
Medicaid prior authorization (PA) policies for treatment of hepatitis C virus (HCV) with direct-acting antiviral (DAA) therapy are changing. We aimed to evaluate effects of changes in PA requirements on treatment uptake and to determine the factors associated with DAA treatment among Florida Medicaid beneficiaries with HCV. This is a retrospective cohort analysis of Florida's Medicaid administrative claims and electronic medical records (2013-2018). A total of 14,063 newly diagnosed patients with HCV were grouped based on human immunodeficiency virus (HIV) co-infection and/or a substance use disorder (SUD) (7,735 HCV mono-infected with a SUD, 5,180 HCV mono-infected without a SUD, 564 HCV/HIV co-infected with a SUD, and 584 HCV/HIV co-infected without a SUD). Although the treatment rate increased three-fold after June 1, 2016, when a fibrosis-stage restriction was eliminated, only 8% received DAAs. Compared to HCV mono-infected without a SUD, HCV mono-infected with a SUD and HCV/HIV co-infected with a SUD were 47% (adjusted hazard ratio, 0.53; 95% confidence interval, 0.47-0.60) and 59% (adjusted hazard ratio, 0.41; 95% confidence interval, 0.28-0.61) less likely to initiate DAAs. Those with HCV/HIV/SUD did not experience a DAA initiation increase after a fibrosis-stage restriction was eliminated. Compared with Whites, Blacks were less likely to receive DAAs but were more likely to complete treatment. Use of medication-assisted therapy was low, despite those on medication-assisted therapy being 60% more likely to initiate DAA therapy and no more likely to discontinue therapy. Despite changes in Florida's Medicaid PA requirements for DAA treatment, only 8% received treatment. Disparities in treatment access were found among patients with HIV and a SUD, and who were Black.
医疗补助(Medicaid)对直接作用抗病毒(DAA)治疗丙型肝炎病毒(HCV)的预先授权(PA)政策正在发生变化。我们旨在评估 PA 要求变化对治疗效果的影响,并确定佛罗里达州医疗补助受益人与 HCV 相关的 DAA 治疗的因素。这是对佛罗里达州医疗补助管理索赔和电子病历(2013-2018 年)的回顾性队列分析。根据人类免疫缺陷病毒(HIV)合并感染和/或物质使用障碍(SUD),共将 14,063 例新诊断的 HCV 患者分为四组(7,735 例 HCV 单感染伴 SUD,5,180 例 HCV 单感染无 SUD,564 例 HCV/HIV 合并感染伴 SUD,584 例 HCV/HIV 合并感染无 SUD)。尽管 2016 年 6 月 1 日消除纤维化分期限制后,治疗率增加了两倍,但只有 8%的患者接受了 DAA 治疗。与 HCV 单感染无 SUD 相比,HCV 单感染伴 SUD 和 HCV/HIV 合并感染伴 SUD 的患者开始 DAA 的可能性分别低 47%(调整后的危险比,0.53;95%置信区间,0.47-0.60)和 59%(调整后的危险比,0.41;95%置信区间,0.28-0.61)。消除纤维化分期限制后,HIV/SUD 患者并未增加 DAA 起始治疗。与白人相比,黑人不太可能接受 DAA 治疗,但更有可能完成治疗。尽管接受药物辅助治疗的患者开始 DAA 治疗的可能性增加了 60%,但药物辅助治疗的使用率仍然很低,且更不可能停止治疗。尽管佛罗里达州医疗补助 DAA 治疗的 PA 要求发生了变化,但只有 8%的患者接受了治疗。在 HIV 和 SUD 患者以及黑人患者中,发现了治疗机会的差异。